


Sequential soft tissue augmentation after occlusal trauma adjustment using clear aligners: a case report
 0
0 Abstract
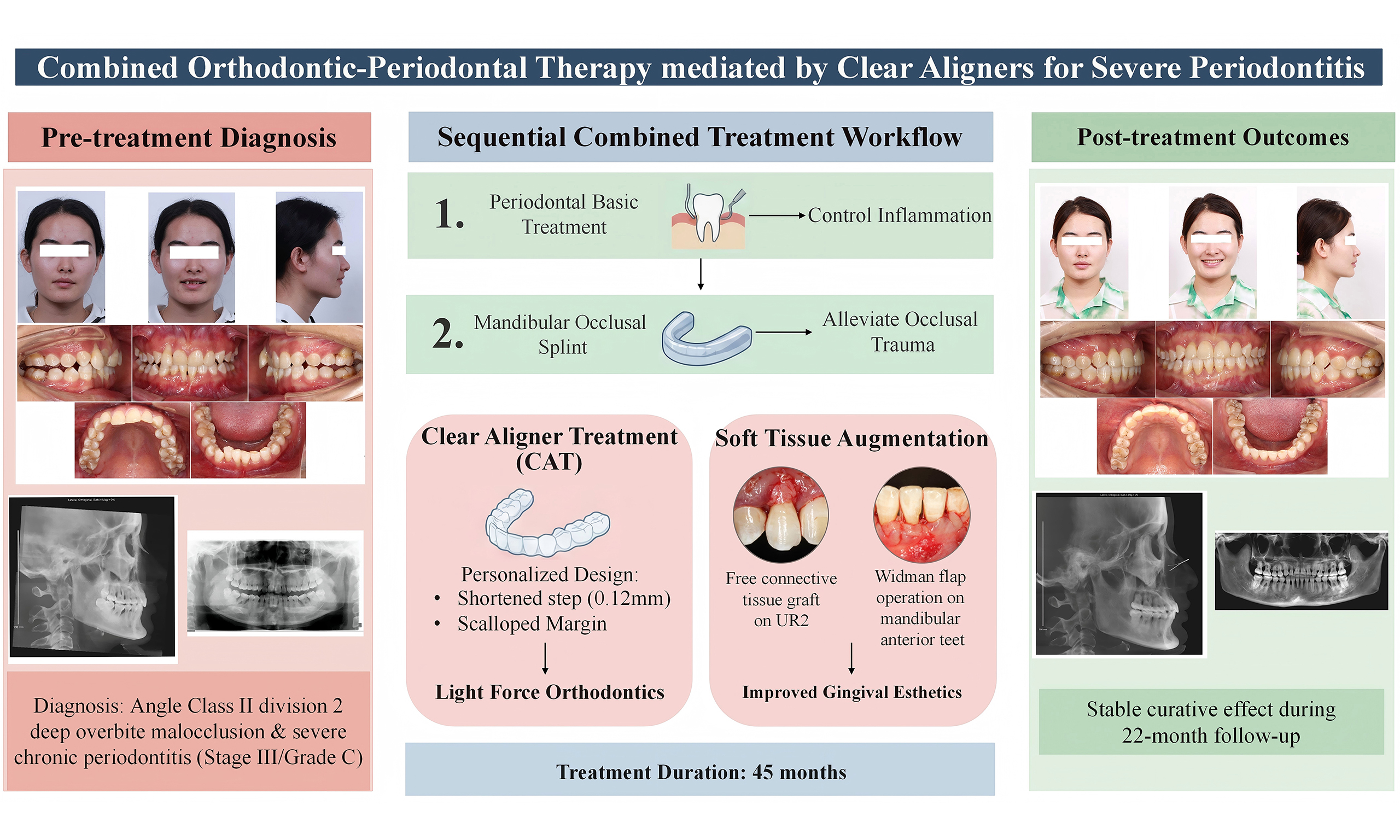
Orthodontic therapy is an important component of a phased periodontal treatment plan. Clear aligners are becoming increasingly used in orthodontics. This case report describes the combined orthodontic-periodontal treatment performed on a 25-year-old female diagnosed with an Angle class II division 2 malocclusion with deep overbite and severe chronic periodontitis (stage III/grade C). The patient received a combination of periodontal therapy and orthodontic treatment with clear aligners. Basic periodontal treatment was used to control plaque and eliminate inflammation, and periodontal surgery was conducted to restore gingival esthetics. For this patient, the combined treatment achieved an ideal occlusal relationship with no progression of periodontal inflammation. Active treatment was completed within 45 months, and the patient was satisfied with both the functional and esthetic outcomes. During the 22-month follow-up, the treatment results remained stable. This case demonstrates that combining clear aligners with periodontal therapy and early relief of occlusal trauma is feasible in patients with periodontal inflammation that is effectively controlled. For selected patients with periodontitis, clear aligners may be a valuable option for improving soft- and hard-tissue esthetics, although this will need confirmation in larger-scale studies.
Keywords
INTRODUCTION
Combining the use of clear aligners (CAs) with periodontal treatment has expanded the scope of CA therapy (CAT) in recent years. Orthodontic treatment is generally carried out after plaque control to inhibit epithelial proliferation and promote the formation of periodontal attachment. However, periodontitis with occlusal trauma requires earlier orthodontic intervention to remove the occlusal trauma and provide time and space for periodontal tissue recovery[1]. Combined orthodontic-periodontal therapy to preserve the affected teeth, restore chewing function, improve smile esthetics and build self-confidence is of particular importance to young patients. CAT is susceptible to complications such as gingival recession, tooth drifting and gingival bleeding if periodontal maintenance is ignored.
The main challenges associated with orthodontic treatment for periodontitis are: (1) precise control of the orthodontic forces[2]; (2) long correction cycle[3]; and (3) requirement for close cooperation between the patient and dentists. The best type of appliance to use for patients with periodontitis remains controversial[4]. Some dentists believe that CAs reduce plaque-retentive factors, favor adequate oral hygiene[5], and reduce the risk of gingivitis progressing to periodontitis. However, other studies have reported that, unlike the continuous light force applied by a fixed appliance[6], a CA drives tooth movement through retainer deformation and exerts an initial force that is notably higher than that of a fixed appliance. Additionally, CA removal and insertion can transmit unfavorable forces to periodontal tissue.
This case report describes the use of CAs to treat severe chronic periodontitis (stage III/grade C) in a patient with Angle class II division 2 malocclusion with deep overbite, who had severe bone resorption and gingival recession of the anterior teeth and four first permanent molars. The treatment included proclination of the anterior teeth to relieve occlusal trauma in combination with a phased periodontal treatment plan [Figure 1].
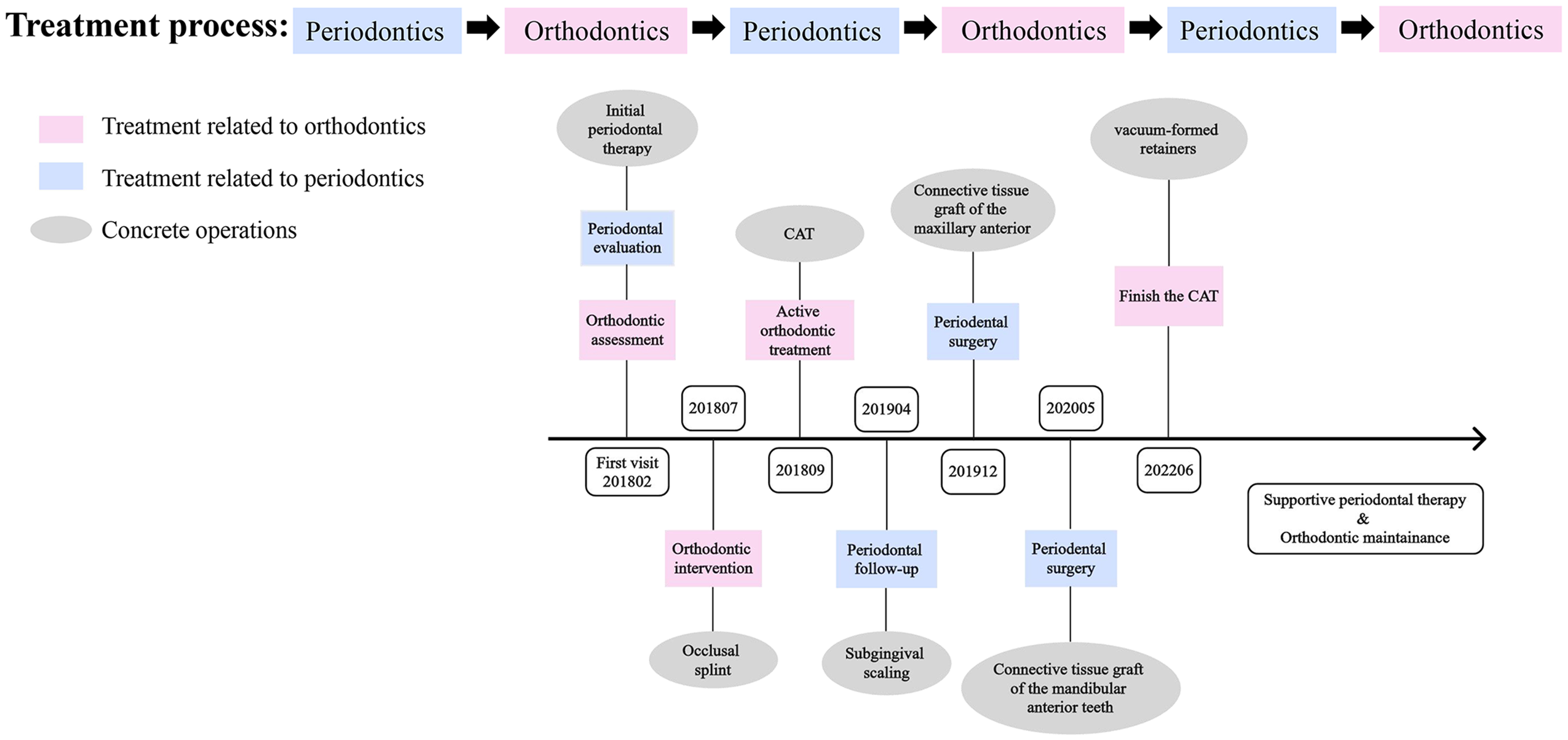
Figure 1. Schematic overview of the combined periodontal and orthodontic therapy used in this case. CAT: Clear aligner therapy.
CASE PRESENTATION
Diagnosis and etiology
This study was approved by the Ethics Committee of The Fourth Military Medical University (IRB-REV-2022163). Written informed consent was obtained from the patient prior to participation in the study. A 25-year-old woman sought treatment for a deep bite and swollen gums at the Department of Orthodontics, Hospital of Stomatology, The Fourth Military Medical University [Figure 2]. Extra-oral examination revealed a straight lateral profile with a decreased lower facial height. The upper and lower lips were located 2 mm behind Ricketts’ E line. The front-smiling photograph revealed severe gingival recession with a proclined right maxillary lateral incisor (UR2). Intra-oral examination demonstrated a deep anterior overbite (4 mm) with heavy occlusal interference. The maxillary anterior teeth were exposed about 3 mm when smiling. Transversely, the mandibular molars showed lingual inclination. The maxillary dental midline deviated by 1 mm to the right relative to the facial midline, whereas the mandibular midline was consistent with the facial midline. Labial dislocation of UR2 and a bilateral class II canine-molar relationship were observed in the sagittal direction. Periodontal examination revealed that the patient had poor oral hygiene and various degrees of gingival recession throughout the dentition. In particular, labial gingival recession was about 4 mm on UR2 and 2 mm on the right mandibular central incisor (LR1), with probing depths ranging from 3-6 mm and grade II-III tooth mobility. The panoramic radiograph showed Grade III horizontal resorption of alveolar bone in the anterior region, Grade II-III angular resorption in the region of the first molars, and Grade I horizontal resorption in the residual teeth. Cephalometric tracing demonstrated a class I skeletal pattern and retroclination of the bimaxillary incisors [Figure 3]. The final diagnosis was class II division 2 malocclusion with a class I skeletal pattern, deep overbite, and stage III grade C periodontitis.

Figure 2. Pre-treatment intraoral photographs, lateral cephalogram, and panoramic radiograph.
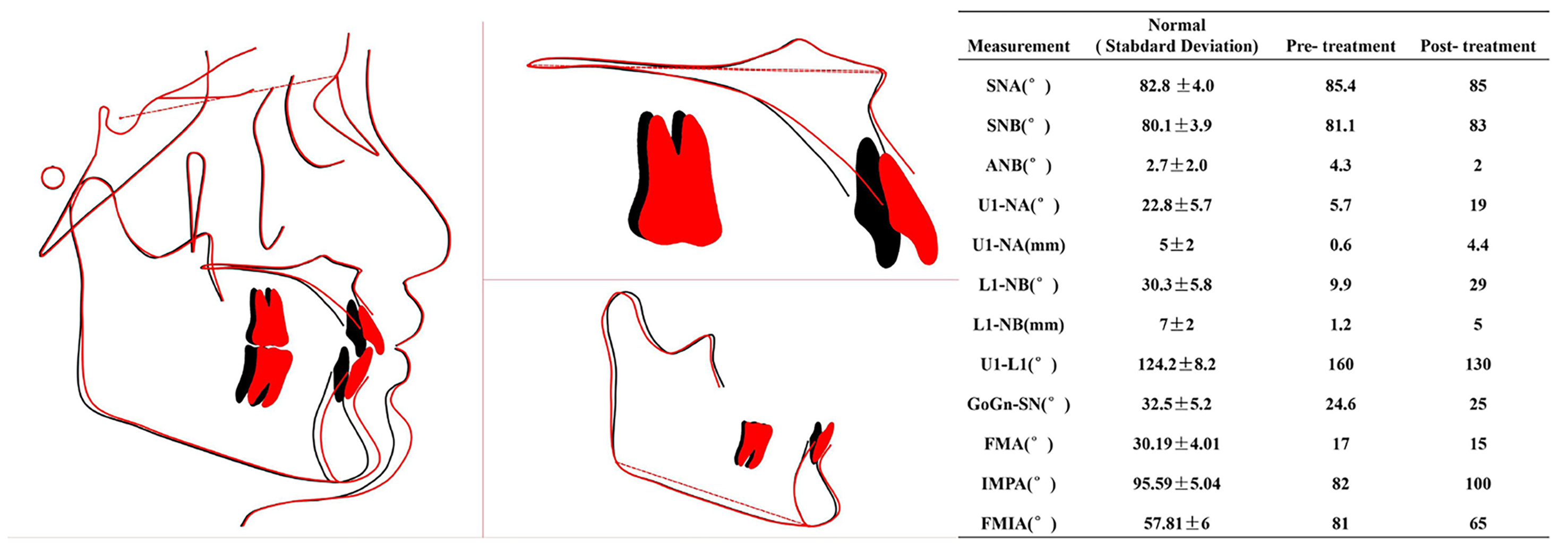
Figure 3. Cephalometric superimposition on the sella-nasion plane registered at the sella and summary of the cephalometric findings. Black line: Pre-treatment; red line: post-treatment. SNA: Sella-nasion-A point angle; SNB: sella-nasion-B point angle; ANB: A point-nasion-B point angle; U1-NA: upper incisor to nasion-A point (angle and distance); L1-NB: lower incisor to nasion-B point (angle and distance); U1-L1: interincisal angle; GoGn-SN: mandibular plane (gonion-gnathion) to sella-nasion plane angle; FMA: Frankfort mandibular plane angle; IMPA: incisor mandibular plane angle; FMIA: Frankfort mandibular incisor angle.
Treatment alternatives
Three interdisciplinary treatment alternatives were planned for this patient after detailed discussions among the members of the multidisciplinary team, and a final decision was made to use inflammation control. The treatment plan alternatives and their advantages and disadvantages are listed in Table 1.
The advantages and disadvantages of all the treatment plan alternatives
| Treatment plan alternatives | Advantages | Disadvantages |
| 1. Extraction of the affected teeth and oral prosthodontics therapy | Short treatment duration | Fixed partial denture: heavy abutment burden Implant restoration: poor long-term stability |
| 2. Retain the affected teeth and fixed orthodontic treatment | Low compliance requirements | Mechanical stimuli; difficulties in maintaining oral hygiene; hard to correct the occlusal trauma |
| 3. Retain the affected teeth and clear aligner treatment | Individualized tooth movement design; Reduce plaque buildup; Pad effect | High compliance requirements |
| Common points: 1. All treatment alternatives focused on the right maxillary lateral incisor and right mandibular central incisor; 2. Orthodontic treatment should be carried out after complete periodontal treatment; 3. Due to the serious absorption of the alveolar bone of the maxillary and mandibular first molars, there was the possibility of extraction. Therefore, the extraction of the third molar was postponed at the beginning, prepared for autogenous tooth transplantation; 4. Regular periodontal visits at interval of two or three months; 5. In order to solve gingival recession of the bimaxillary anterior teeth, mucogingival surgery was necessary | ||
The Invisalign system was used for customized design and adjustment of the CAs. The following measures were used to maximize the benefits of CAT. First, a mandibular occlusal splint was used for three months after periodontal treatment to allow the patient to become familiar with the usage of the appliance while alleviating occlusal trauma. Second, the linear displacement (step size) was shortened to 0.12 mm per aligner, and the torque movement was set to 0.5° per aligner, to prevent an excessive initial force. Furthermore, the gingival margin of the retainers was cut down to the enamel-cementum junction, and no attachment was used.
Treatment procedure
The patient was referred to the periodontal department for supragingival scaling and root planing, and internal scaling of the molars was performed at the follow-up appointment three months later [Figure 4A]. At this time, an occlusal splint was made for the mandibular dentition to remove occlusal trauma. Three months later, the inflammation was well controlled, and orthodontic therapy was officially started [Figure 4B].
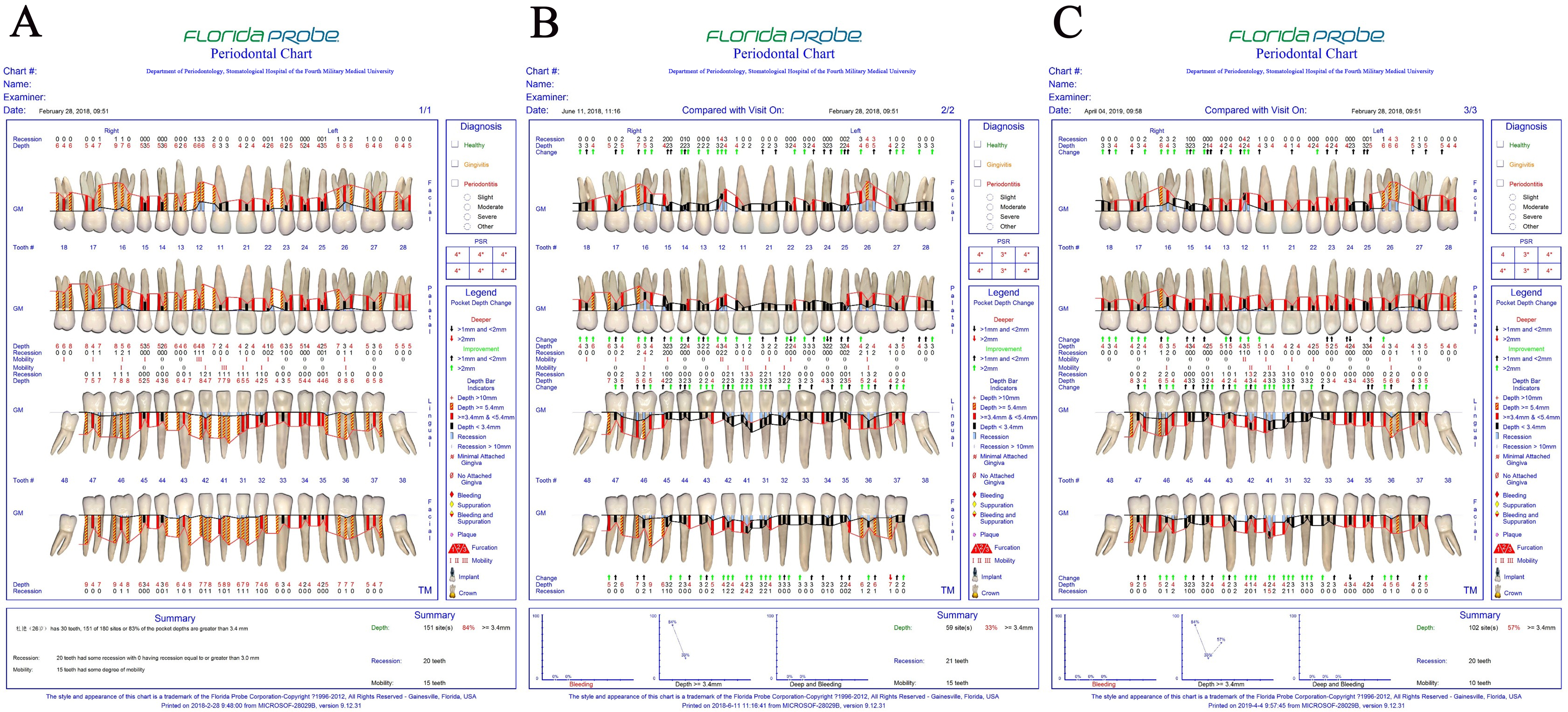
Figure 4. The results of probing depth measurements. (A) At the first visit to the periodontist, the anterior teeth and first molars had deep periodontal pockets; (B) Three months after the initial periodontal therapy, the inflammation was well controlled; (C) Periodontal inflammation recurred during the first period of orthodontic therapy, and scaling and root planing were performed again.
The orthodontic treatment was carried out over three time periods, with 67 aligners used for the first period. The displacement step for each aligner was reduced from 0.25 to 0.12 mm, while the torque step was set to 0.5°. The main goal of this period was to align and level the bimaxillary anterior teeth, relieve occlusal trauma, and prepare the patient for later periodontal surgery. At the 11th aligner stage, the anterior teeth were effectively proclined, but the proportion of periodontal probing sites > 4 mm had increased from 33% to 57%, indicating a recurrence of periodontal inflammation that necessitated repeat scaling and root planing [Figure 4C]. At the 38th aligner stage, the plaque was well controlled, and the gingival inflammation had essentially subsided. At the end of this first period, the anterior teeth were satisfactorily aligned, and the occlusal trauma had been relieved. However, gingival recession of the anterior teeth was the main factor affecting the esthetic.
Periodontal surgery was planned after consultation with the periodontist to further improve the gingival esthetics of the anterior region. Free connective tissue graft - a procedure where tissue is harvested from the palate and transplanted to cover an exposed root surface to augment soft tissue thickness and improve esthetics - was performed on UR2 [Figure 5A]. A tissue graft (8 mm × 8 mm) was harvested from the palatal area [Figure 5B] and transplanted onto the coronal part of the recessed area, and the gingival margin was trimmed slightly higher than the adjacent teeth [Figure 5C]. One month after the operation, the wound had healed well, the mobility of UR2 had improved, and the gingival margin was at the same level as that of the adjacent teeth [Figure 5D]. CAs continued to be worn after surgery.
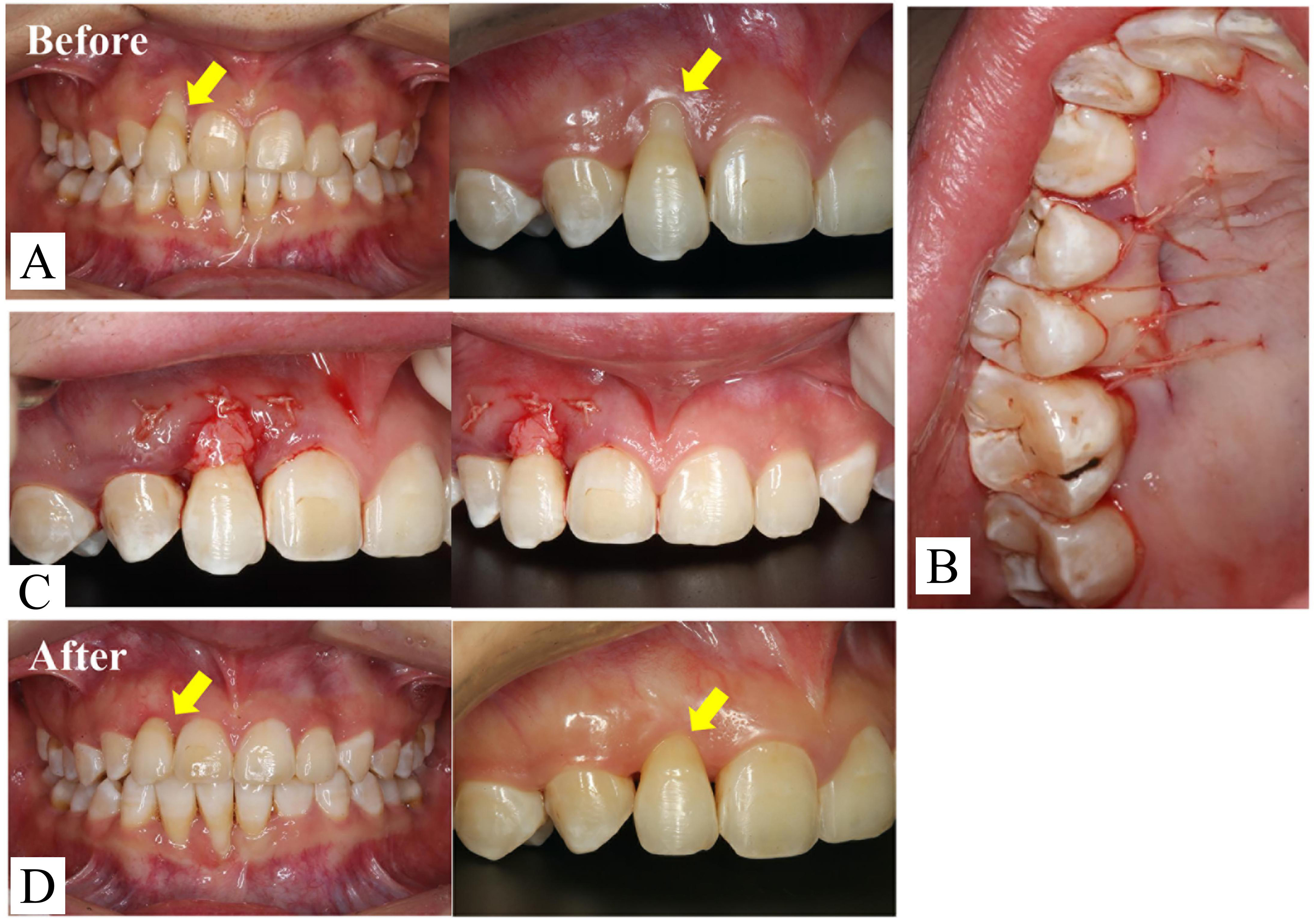
Figure 5. Mucogingival surgery of the maxillary anterior teeth. (A) Pre-surgery intraoral photographs showing severe gingival recession; (B) A free soft tissue graft was obtained from the maxillopalatine side; (C) Intraoperative intraoral photographs; (D) One month after surgery, the gingival margin of the lateral incisor was almost at the same level as that of the adjacent teeth.
Exposure of the root surface of LR1 was dealt with after 4 months. The Widman flap operation - a modified periodontal surgical technique that involves creating precise incisions to reflect a flap of gingiva, allowing direct visualization and thorough debridement of the root surface and alveolar bone while maximally preserving healthy tissue - was performed on the mandibular anterior teeth [Figure 6A-D]. A free connective tissue graft was transplanted, and a coronal reduction and suspension suture were performed [Figure 6E]. The wound healed well, with normalization of the shape of the gingival margin and substantial improvement in the root surface exposure [Figure 6F and G].
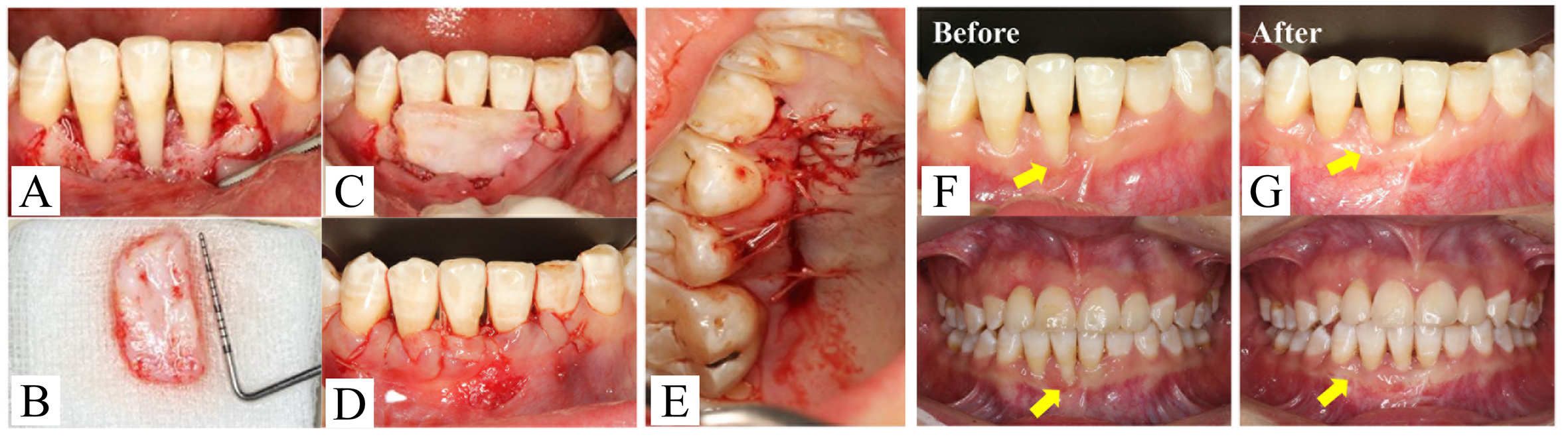
Figure 6. Mucogingival surgery of the mandibular anterior teeth. (A-D) Treatment procedures for the connective tissue graft and coronally advanced flap; (E) Palatal donor area of the free soft tissue graft; (F and G) Intraoral photographs before and two months after surgery.
The objective of the first period was achieved at the 60th aligner stage, with the patient exhibiting normal overbite and overjet and a class I bilateral sagittal occlusal relationship. Periodontal surgery had stabilized the affected teeth. The goal of the next period was to extrude UR3, buccally tip the mandibular posterior teeth, and close the posterior open bite by controlling the posterior vertical dimension. After 31 sets of aligners had been used, the bilateral posterior open bite had resolved, and the vertical position of the right upper canine was ideal. The occlusal relationship was finely adjusted during the second restart. Thirty-five sets of aligners were designed to buccally tilt the mandibular second molars, and a small amount of lingual movement of the lower anterior teeth was implemented to prevent occlusal trauma. Supportive periodontal therapy was a prerequisite for long-term maintenance and was administered throughout the entire period of orthodontic treatment.
RESULTS
After 45 months of treatment, the bilateral molar and canine relationships reached class I, and the posterior teeth were tightly occluded. The anterior occlusal trauma and deep overbite had been corrected. Sequential treatment of periodontal disease had resulted in the gingival inflammation being well controlled, and the smile esthetics were attractive [Figure 7].

Figure 7. Post-treatment intraoral photographs, lateral cephalogram, and panoramic radiograph.
CASE RETENTION
In order to prevent a relapse of malocclusion, Super-Bond (4-META/MMA-TBB resin) was applied permanently around the bimaxillary anterior teeth near the surgical field. Vacuum-formed retainers (membrane thickness: 0.8 mm) that covered only half of the tooth crown were used every other night to maintain the treatment effect, and regular reexamination was recommended every 6 months [Figure 8].
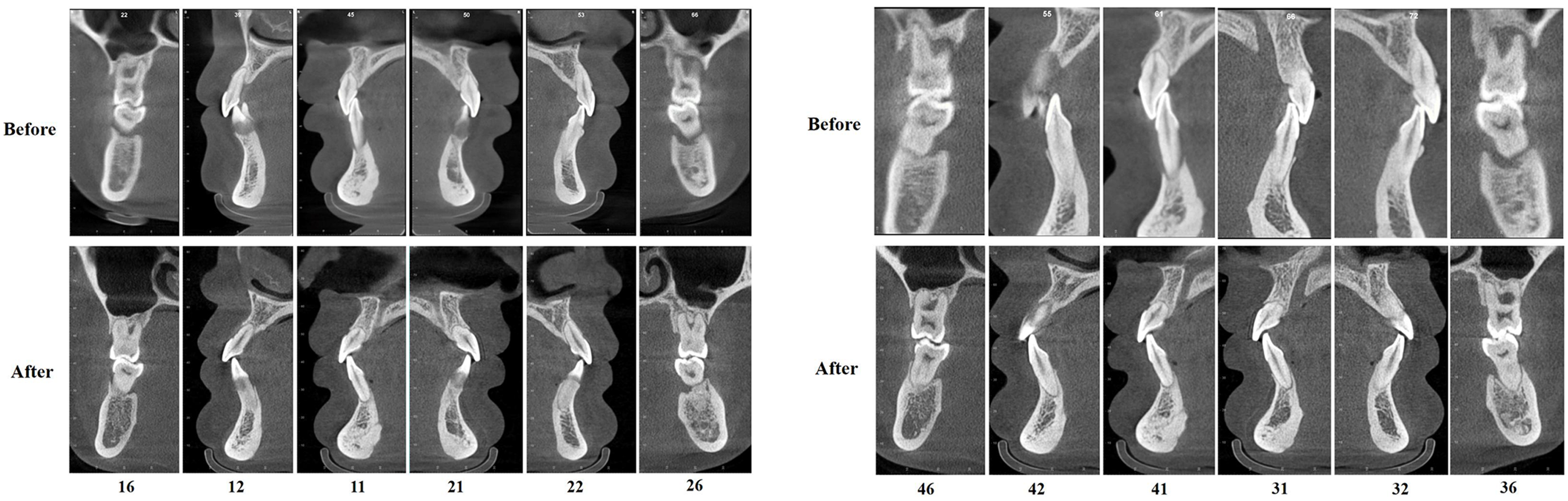
Figure 8. The labiolingual cortex of the bimaxillary anterior teeth in the sagittal view. The maxillary anterior teeth stood upright in the alveolar bone. Occlusal trauma was no longer present, and no obvious worsening of alveolar resorption was evident.
Cephalometric superimposition confirmed that the anterior teeth were well aligned with a normal torque [Figure 3]. The improvement in gingival esthetics led to increased self-confidence and a fuller and more harmonized smile. The patient’s periodontal condition and occlusal relationship were stable at the 22-month return visit, and she was very satisfied with the therapeutic results [Figure 9].

Figure 9. Facial and intraoral photographs after 22-month retention. The patient exhibited an attractive smile, and the treatment effect was stable.
DISCUSSION
Selection of the treatment protocol
This patient was diagnosed with Angle class II division 2 malocclusion with deep overbite and severe chronic periodontitis (stage III/grade C). The treatment objectives were not only to improve dental alignment and esthetics but also, more crucially, to promptly control and eliminate the persistent damage to periodontal supporting tissues caused by the abnormal occlusal load. Therefore, after weighing the patient’s individual clinical conditions and personal wishes, the decision was made to adopt a protocol combining CAT, sequential soft tissue augmentation and sequential periodontal therapy.
When compared with conventional combination therapy comprising fixed orthodontics and periodontal treatment, CAT offers advantages in oral hygiene maintenance[7] and superior vertical control with its full-coverage design and “bite block effect”[8]. The bite block effect can rapidly open the bite and alleviate the damage to periodontal tissues caused by traumatic occlusion. Research by Chen et al. confirmed that sequential hard and soft tissue augmentation following the elimination of traumatic occlusion with CAT is an effective protocol for improving the level of periodontal supporting tissues[9]. In addition, for cases with a poor periodontal condition, slowing down the rate of tooth movement and reducing the dental coverage of aligners help to lower periodontal risks. Thus, CAs are recommended for patients who are susceptible to gingivitis and/or periodontitis[10]. Based on this principle, CAT was selected for this patient: the tooth movement step was reduced to 0.12 mm, and the edges of the aligners were finely trimmed to avoid secondary damage to the periodontium.
However, while periodontal stabilization therapy alone is capable of controlling inflammation, it fails to address malocclusion and traumatic occlusion. Although this approach may be suitable for patients unable to comply with more intensive treatment regimens, it is associated with a poorer long-term prognosis. In cases characterized by persistent occlusal trauma or pathologic tooth migration, managing inflammation without correcting the underlying malocclusion is insufficient to achieve functional recovery and ensure long-term stability[11,12]. Extraction followed by prosthetic rehabilitation is indicated for teeth with an extremely poor prognosis, limited preservation value, or when the dentition cannot be maintained otherwise. This approach necessitates sacrifice of natural teeth and entails long-term maintenance costs associated with the prosthesis[13,14].
Appropriate timing of treatment for patients with malocclusion and periodontitis
Periodontitis is the most common chronic noninfectious inflammatory disease in humans[15] and the primary cause of tooth loss in adults. Periodontitis requires early intervention such as basic and surgical periodontal treatment. There is increasing evidence that under close periodontal maintenance therapy, orthodontic treatment has little influence on the clinical attachment level (a core clinical metric quantifying the loss of tooth-supporting tissues) and that clinical indicators related to periodontitis do not significantly worsen after orthodontic treatment[16]. However, the timing of orthodontic treatment in a patient with periodontitis remains a controversial issue[17]. Xie et al. deemed that orthodontic treatment should be considered when the plaque index is < 25%, bleeding on probing sites is < 30%, and there are no deep periodontal pockets larger than 5 mm[18]. Some studies have pointed out that orthodontic treatment should be individually designed according to the type of periodontal treatment; for example, flap surgery should be started after 6-9 months, while guided tissue regeneration should be delayed until 1 year later[17].
In this patient, there was obvious occlusal trauma to LR1, and the accompanying local inflammation was able to progress to the root easily, resulting in vertical absorption of alveolar bone; hence, early orthodontic treatment was required to eliminate the occlusal trauma. The patient chose to undergo orthodontic and periodontal treatment at the same time, and the final treatment effect was excellent. Regular periodontal examination was considered essential during the orthodontic procedure. After 7 months of orthodontic therapy, the proportion of sites with a probing depth > 4 mm had increased, so supragingival scaling, scaling and root planing were performed immediately to control the inflammation and ensure that it did not affect the overall benefits of orthodontic treatment.
Suggestions for orthodontic treatment of patients with periodontitis
Applying appropriate orthodontic force promotes the reconstruction and regeneration of periodontal tissue. Reducing the moving distance of each aligner tray decreases the force applied to the teeth. An experiment in beagle dogs showed that the elastic modulus of the periodontal membrane was maximal when the step distance was 0.35 mm and that maximum efficiency could be achieved without damaging the health of the periodontal tissue[2]. A finite element study concluded that the CA steps should not exceed 0.18 mm for a normal alveolar ridge, 0.15 mm when there is absorption of one-third of the bone, and 0.10 mm when there is absorption of two-thirds of the bone[19]. In this case, UR2 and LR1 had degree III alveolar bone resorption, the four first molars had degree II-III angular resorption in the lower posterior region, and the remaining teeth exhibited degree I horizontal resorption. Given this, the moving distance of each aligner was reduced from 0.25 to 0.12 mm, and a satisfactory treatment effect was obtained.
An increase in the size and number of attachments is conducive to aligner fixation. It has been suggested that a higher number of attachments on the anterior teeth is a risk factor for the development of black gingival triangles. For example, a prior study found that the proportion of patients with more than two attachments on each anterior tooth was higher in the group with black gingival triangles than in those without[20]. Since the periodontal condition of the patient reported here was poor at the initiation of treatment, aligners were designed with no attachments during the first stage in order to reduce the orthodontic forces and stimulation of periodontal tissue during removal.
The shape and height of the gingival margin of a CA affects periodontal tissue health. The longer the edge of the aligner, the closer the force is to the resistant center of the tooth, and the easier it is to generate bodily movement. However, a longer edge also increases the stress on the neck of the crown. The finite element study of Lyu et al. showed that extension of the gingival margin of an aligner led to stress being concentrated on the crown of the tooth and that a linear margin produced greater stress on the crown neck than a scalloped margin[21]. When we submitted the prescription for the present case in the Invisalign system, we explicitly specified in the design notes that the trim line should be a scalloped margin that followed the gingival scalloped margin, positioned approximately 2 mm coronal to the cemento-enamel junction. Chairside trimming was performed during treatment if the margin was considered excessively long, and the patient was instructed from the outset to monitor the edge length.
A retention procedure is necessary to maintain the corrected positions of the teeth following active orthodontic treatment. Vacuum-formed, permanent lingual and partial Super-Bond retainers are commonly used in clinical practice. The force generated when a vacuum-formed retainer is inserted or removed can be harmful to delicate periodontal tissue[22]. A permanent lingual retainer is similar to a periodontal splint but is easily broken and hard to clean. A Super-Bond retainer is invisible and particularly suitable for partial retention after periodontal surgery. In this case, we used Super-Bond in combination with vacuum-formed retainers as the final retention protocol to maintain the corrected position of the teeth without injuring the periodontal tissue.
Smile esthetics in patients with periodontitis
The amount of gum and tooth exposure during a smile plays an important role in the dynamic esthetics of the face. In the present case, the main reasons for the poor appearance of the patient’s smile before treatment were labial displacement of UR2 and gingival recession. Three membrane-gingival operations, namely the lateral transposition flap technique, the coronally advanced flap technique and free connective tissue transplantation, are commonly performed to repair periodontal soft tissue defects. The lateral transposition flap and coronally advanced flap techniques are both established and effective for Miller class I and II gingival recession[23]. In the present case, it was difficult to achieve tension-free gingival graft reduction and long-term stability using these two surgical procedures alone because the proximal alveolar bone of the patient’s UR2 and LR1 had angular absorption to one-third of the root tip. Therefore, following basic periodontal treatment, free connective tissue graft for UR2 and LR1 was combined with the coronally advanced flap technique in a stepwise manner. One study demonstrated that a palatal free tissue graft harvested with periosteum can form long junctional epithelium between exposed roots, artificially establishing biological width, blocking the path for bacterial invasion into periodontal tissue, reducing the accumulation of subgingival plaque, and possibly providing an attachment for the growth of alveolar bone[24].
Monitoring and support strategies for patient compliance
The effectiveness of a CA relies on it being worn consistently for at least 22 h per day, which imposes high demands on patient cooperation[25]. Furthermore, individuals with poor oral hygiene are more susceptible to periodontal inflammation during CAT[26]. Therefore, the success of this treatment is highly dependent on patient compliance. Poor compliance - such as insufficient wear time, inadequate maintenance of oral hygiene, or unauthorized interruption of follow-up visits - can result in reduced tooth movement efficiency, recurrence of periodontal inflammation, compromised treatment outcomes and poorer long-term prognosis. To address this potential issue, the following strategies were implemented to enhance patient compliance: (1) pre-treatment education regarding the consequences of poor compliance; (2) remote monitoring of wear time and positive reinforcement for patients using relevant applications; and (3) timely reminders sent to patients when non-compliant behaviors were detected during treatment[25].
Cost-benefit analysis
This treatment protocol involves complex procedures and relatively high costs with considerable demands on institutional equipment (e.g., digital orthodontic design systems and periodontal surgical instruments) and clinician expertise. Consequently, its implementation is limited to medical institutions capable of delivering integrated periodontal and orthodontic care, which to some extent restricts its accessibility in primary care settings and broader community outreach. Regarding treatment costs, neither CAT nor soft tissue augmentation procedures are currently covered by medical insurance, posing a major barrier for many patients seeking this treatment. Nevertheless, although this protocol entails higher upfront costs than alternative approaches, it addresses the core issues at their source and reduces the need for subsequent management of complications and prosthetic maintenance, thereby offering superior long-term cost-effectiveness[13,14]. This combined approach may yield long-term benefits in patients with good compliance, in whom periodontal inflammation can be stably controlled, enabling the treatment goal to be preservation of the natural teeth and functional rehabilitation. Conversely, priority should be given to simpler alternative treatment protocols in patients unable to adhere to long-term sequential treatment.
LIMITATIONS
This case report has certain limitations. First, there is an obvious case selection bias: the study subject was a young adult with severe chronic periodontitis (stage III/grade C) complicated by Angle class II division 2 malocclusion, so the results may not be generalizable to elderly patients or those with periodontitis of different grades or other types of malocclusion. Second, the follow-up duration was short (only 22 months), which is insufficient for evaluation of the long-term efficacy of this intensive periodontal-orthodontic combination treatment. Potential complications such as recurrent periodontal inflammation and progressive alveolar bone resorption during long-term follow-up cannot be completely ruled out, and prolonged follow-up is needed to verify the long-term stability of the therapeutic effect. In addition, despite favorable clinical and imaging outcomes, objective quantitative detection of periodontal regeneration (e.g., re-probing or cone-beam computed tomography-based quantitative measurement of relevant alveolar bone indicators) was not performed, precluding full evaluation of periodontal treatment efficacy and the effect of combination therapy on periodontal regeneration. Finally, this is a single case report, and future case series and controlled clinical trials are required to further evaluate the reproducibility of CAT, long-term periodontal health status, and therapeutic differences between CAT and fixed orthodontic treatment.
CONCLUSIONS
This case report detailed the combined orthodontic-periodontal therapy of an adult female with severe chronic periodontitis (stage III/grade C) and class II division 2 malocclusion with deep overbite. The ideal result was achieved through a personalized treatment design and rigorous sequential periodontal treatment. The findings of this case preliminarily suggest that, for carefully selected patients with severe chronic periodontitis whose periodontal inflammation has been effectively controlled, it is feasible to implement CAT in combination with sequential periodontal treatment under the principle of applying small orthodontic forces. This case provides a practical reference for the clinical management of patients with severe chronic periodontitis complicated by malocclusion, although further research in a larger population is needed to verify these findings.
DECLARATIONS
Authors’ contributions
Contributed to conceptualization, the literature review and writing of the case report: Wang Y
Contributed to writing of the case report: Qiang R
Contributed to the literature review: Gan D
Contributed to the treatment of the patient and critical reviewing of the case report: Miao H
Contributed to the treatment of the patient, reviewing of the case report, and funding acquisition: Gao J
Availability of data and materials
The data underlying this article will be shared on reasonable request to the corresponding author.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This work was supported by grant (LCB202202, LCA202203, LCA202403) from the National Clinical Research Center for Oral Diseases, grant (CSA-02022-01) from the CSA Clinical Research Fund, grant (A2023-13) from the China Oral Health Foundation, grant (LX2022-401) from the New Technologies and New Business of School of Stomatology, The Fourth Military Medical University Fund, and grant (2025TD-15) from Innovation Team of the Health Commission of Shaanxi Province.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was approved by the Ethics Committee of The Fourth Military Medical University (IRB-REV-2022163). Written informed consent was obtained from the patient prior to participation in the study.
Consent for publication
Informed consent for the publication of the patient’s images has been obtained.
Copyright
© The Author(s) 2026.
REFERENCES
1. Laursen MG, Rylev M, Melsen B. The role of orthodontics in the repair of gingival recessions. Am J Orthod Dentofacial Orthop. 2020;157:29-34.
2. Wang Y, Chen J, Qin S, et al. An in vivo evaluation of clear aligners for optimal orthodontic force and movement to determine high-efficacy and periodontal-friendly aligner staging. Heliyon. 2023;9:e15317.
3. Son HJ, Lee KH, Sim JY, Kim HY, Kim JH, Kim WC. Pressure differences from clear aligner movements assessed by pressure sensors. Biomed Res Int. 2020;2020:8376395.
4. Rouzi M, Jiang Q, Zhang H, Li X, Long H, Lai W. Characteristics of oral microbiota and oral health in the patients treated with clear aligners: a prospective study. Clin Oral Investig. 2023;27:6725-34.
5. Barreda GJ, Dzierewianko EA, Mazza V, Muñoz KA, Piccoli GI, Romanelli HJ. Expansion treatment using Invisalign®: periodontal health status and maxillary buccal bone changes. A clinical and tomographic evaluation. Acta Odontol Latinoam. 2020;33:69-81.
6. Ke Y, Zhu Y, Zhu M. A comparison of treatment effectiveness between clear aligner and fixed appliance therapies. BMC Oral Health. 2019;19:24.
7. Dipalma G, Inchingolo AD, Fiore A, et al. The differential impact of clear aligners and fixed orthodontic appliances on periodontal health: a systematic review. Children. 2025;12:138.
8. Dipalma G, Marinelli G, Inchingolo F, et al. Clinical efficacy of clear aligners in class II malocclusion: from pediatric to adult cases-a narrative review. J Funct Biomater. 2025;16:354.
9. Chen M, Chen X, Sun L, Zhao B, Liu Y. Sequential soft- and hard-tissue augmentation after clear aligner-mediated adjustment of traumatic occlusion: a case report. J Am Dent Assoc. 2022;153:572-81.e1.
10. Wang Y, Long H, Zhao Z, et al. Expert consensus on the clinical strategies for orthodontic treatment with clear aligners. Int J Oral Sci. 2025;17:19.
11. Zasčiurinskienė E, Rastokaitė L, Lindsten R, Basevičienė N, Šidlauskas A. Malocclusions, pathologic tooth migration, and the need for orthodontic treatment in subjects with stage III-IV periodontitis. A cross-sectional study. Eur J Orthod. 2023;45:418-29.
12. Miao S, Wu Y, Ning H, Xu J. An observational study of the efficacy of combined orthodontic-systemic periodontal treatment. Medicine. 2025;104:e43373.
13. Afrashtehfar KI, Assery NM, Alblooshi KAK, Schmidlin PR. Maintaining periodontally compromised teeth seems more cost-effective than replacing them with dental implants. Evid Based Dent. 2024;25:129-30.
14. Nagpal D, Ibraimova L, Ohinmaa A, Levin L. The cost-effectiveness of tooth preservation vs implant placement in severe periodontal disease patients: a systematic review. Quintessence Int. 2024;55:76-85.
15. Herrera D, Berglundh T, Schwarz F, et al; EFP workshop participants and methodological consultant. Prevention and treatment of peri-implant diseases-The EFP S3 level clinical practice guideline. J Clin Periodontol. 2023;50:4-76.
16. Martin C, Celis B, Ambrosio N, Bollain J, Antonoglou GN, Figuero E. Effect of orthodontic therapy in periodontitis and non-periodontitis patients: a systematic review with meta-analysis. J Clin Periodontol. 2022;49:72-101.
17. Pini Prato GP, Chambrone L. Orthodontic treatment in periodontal patients: the use of periodontal gold standards to overcome the “grey zone”. J Periodontol. 2020;91:437-41.
18. Xie Y, Zhao Q, Tan Z, Yang S. Orthodontic treatment in a periodontal patient with pathologic migration of anterior teeth. Am J Orthod Dentofacial Orthop. 2014;145:685-93.
19. Ma Y, Li S. The optimal orthodontic displacement of clear aligner for mild, moderate and severe periodontal conditions: an in vitro study in a periodontally compromised individual using the finite element model. BMC Oral Health. 2021;21:109.
20. Zhang Y, Wang X, Wang J, et al. IPR treatment and attachments design in clear aligner therapy and risk of open gingival embrasures in adults. Prog Orthod. 2023;24:1.
21. Lyu X, Cao X, Yan J, Zeng R, Tan J. Biomechanical effects of clear aligners with different thicknesses and gingival-margin morphology for appliance design optimization. Am J Orthod Dentofacial Orthop. 2023;164:239-52.
22. Li B, Lu C, Yao X, Wu X, Wu G, Zeng X. Effects of three orthodontic retainers on periodontal pathogens and periodontal parameters. Sci Rep. 2023;13:20709.
23. Sharma P, Vaish S, Sharma N, Sekhar V, Achom M, Khan F. Comparative evaluation of efficacy of subepithelial connective tissue graft versus platelet-rich fibrin membrane in surgical reconstruction of interdental papillae using Han and Takie technique: a randomized controlled clinical trial. J Indian Soc Periodontol. 2020;24:547-53.
24. Goldstein M, Boyan BD, Cochran DL, Schwartz Z. Human histology of new attachment after root coverage using subepithelial connective tissue graft. J Clin Periodontol. 2001;28:657-62.
25. Timm LH, Farrag G, Baxmann M, Schwendicke F. Factors influencing patient compliance during clear aligner therapy: a retrospective cohort study. J Clin Med. 2021;10:3103.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].