


Helicobacter pylori is associated with a higher risk of MAFLD prevalence and all-cause mortality: results from the NHANES III follow-up study
 0
0 Abstract
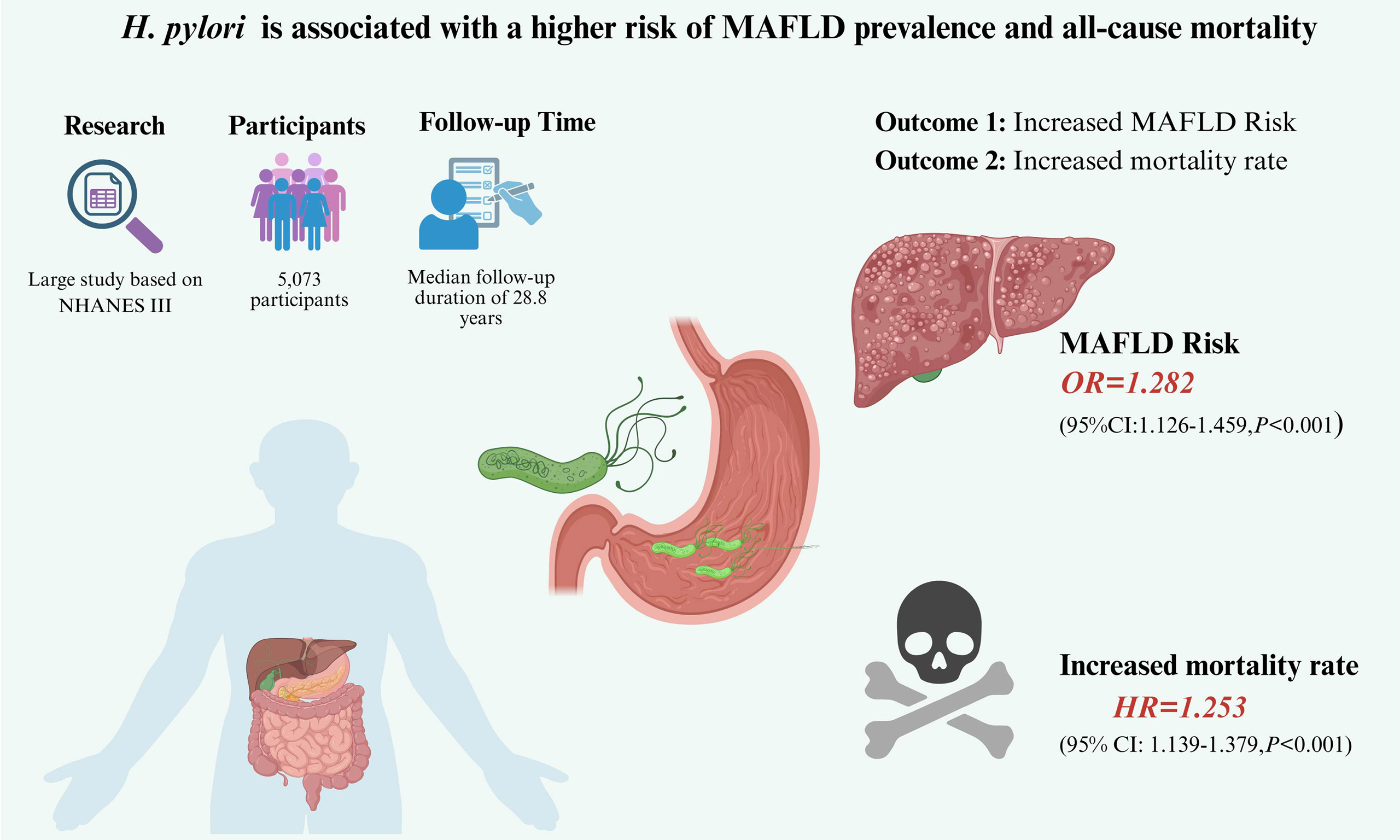
Aim: This study examined the relationship between Helicobacter pylori (H. pylori) and metabolic dysfunction-associated fatty liver disease (MAFLD) and concurrently evaluated their association with all-cause mortality risk.
Methods: Data were extracted from the Third National Health and Nutrition Examination Survey, which included 5,073 participants with available H. pylori IgG serology [enzyme-linked immunosorbent assay (ELISA)] results and mortality data. Logistic regression was used to assess the relationship between H. pylori seropositivity and MAFLD risk, while Cox proportional hazards regression was used to evaluate all-cause mortality risk, with adjustment for confounders.
Results: Among 5,073 participants, 2,394 (47.2%) tested positive for H. pylori and 1,610 (31.7%) had MAFLD; during a median follow-up of 28.8 years, 1,891 deaths occurred (overall mortality rate 37.3%). H. pylori-seropositive individuals exhibited significantly higher mortality rates than seronegative individuals (43.5% vs. 31.7%, P < 0.001). Multivariate logistic regression confirmed H. pylori seropositivity as an independent risk factor for MAFLD [adjusted odds ratio (OR) = 1.282, 95% confidence interval (CI): 1.126-1.459, P < 0.001]. Multivariate Cox regression revealed that H. pylori seropositivity independently increased mortality risk (adjusted HR = 1.253, 95%CI: 1.139-1.379, P < 0.001), which was consistent across the MAFLD and non-MAFLD subgroups. Kaplan-Meier analysis corroborated significant survival divergence (log-rank, P < 0.001).
Conclusion: This study indicates that H. pylori seropositivity is independently associated with a higher prevalence of MAFLD and greater mortality risk in community-dwelling individuals.
Keywords
INTRODUCTION
Helicobacter pylori (H. pylori) is a highly prevalent bacterial pathogen, affecting over 50% of the global population[1]. H. pylori infection is not only associated with a higher incidence of several gastric diseases, such as chronic gastritis, peptic ulcer disease, and gastric cancer[2], but also contributes to the risk of extragastric disorders[3]. Notably, H. pylori infection has been identified as a risk factor for cardiovascular diseases (e.g., coronary heart disease, arrhythmia, and acute myocardial infarction)[4], hepatobiliary system tumors and gallstones[5], as well as cholelithiasis[6]. The high global prevalence of H. pylori infection imposes a significant economic burden on national economies.
Metabolic dysfunction-associated fatty liver disease (MAFLD), a condition redefined to emphasize metabolic risk factors, has emerged as a “silent epidemic”[7]. The overall prevalence of MAFLD worldwide is estimated to be 32.4%[8], aligning with global trends projecting over 100 million cases in the U.S. by 2030[9]. Accumulating evidence indicates that MAFLD markedly increases the risk of liver fibrosis, cirrhosis, and hepatocellular carcinoma, particularly in individuals with comorbid metabolic disorders such as insulin resistance and obesity[10]. Moreover, MAFLD is associated with an increased incidence of extrahepatic conditions, including cardiovascular diseases[11], neurological disorders, and diverse malignancies beyond the liver, such as colorectal and breast cancer[12].
Recognition of the gut microbiome’s contribution to MAFLD has shifted attention toward the role of
Therefore, this study utilized the Third National Health and Nutrition Examination Survey (NHANES III) database to conduct a cross-sectional analysis to investigate the potential relationships among H. pylori seropositivity, MAFLD, and all-cause mortality risk.
METHODS
Study population
NHANES III (1988-1994), a nationally representative survey coordinated by the Centers for Disease Control and Prevention’s (CDC’s) National Center for Health Statistics (NCHS), provided the data for this study. De-identified data were retrieved from the CDC’s public repository (https://wwwn.cdc.gov/nchs/nhanes/) following the protocols for the secondary analysis of population-based health surveys. We included adult participants (age ≥ 20 years) from the NHANES III (1988-1994) with complete data on H. pylori IgG serology and hepatic ultrasonography. Participants with missing baseline anthropometric data or incomplete follow-up information in the NHANES III Linked Mortality File were excluded. Mortality outcomes through December 2019 were acquired from the National Death Index (NDI) linkage files (updated May 2022), using probabilistic matching of participant identifiers (https://ftp.cdc.gov/pub/Health_Statistics/NCHS/datalinkage/linked_mortality/). The original NHANES III protocol was approved by the NCHS Research Ethics Review Board, and written informed consent was obtained from all participants. Given that only anonymized, publicly available data were used, an individual ethics review was not required.
Definition
MAFLD
Hepatic steatosis was assessed using ultrasonography as the primary radiological modality. Data from two separate ultrasound examinations obtained from the NHANES III database were combined to form a unified analytical dataset. The severity of hepatic steatosis, determined using standard ultrasonographic criteria, was categorized as normal (no fat deposition), mild, moderate, or severe. For analytical purposes, cases exhibiting mild, moderate, or severe steatosis were grouped and classified as having clinically significant hepatic steatosis. MAFLD diagnosis adhered to the criteria specified in a recent international expert consensus[17]. This diagnostic framework mandates ultrasonographic evidence of hepatic steatosis coupled with the presence of at least one additional criterion: (1) overweight or obesity [body mass index (BMI) ≥ 25 kg/m2]; (2) type 2 diabetes mellitus; or (3), in non-obese individuals (BMI < 25 kg/m2), the presence of two or more metabolic risk abnormalities. For the NHANES III, race was classified into four distinct categories: non-Hispanic White, non-Hispanic Black, Mexican American, and Other.
H. pylori antibody test
Serological detection of H. pylori IgG antibodies was performed using a commercial enzyme-linked immunosorbent assay (ELISA) kit[18], following the manufacturer’s instructions. This ELISA is designed for qualitative detection of H. pylori IgG in human serum and has demonstrated sensitivity, specificity, and reproducibility comparable to established serological techniques[19].
Operational definitions
Type 2 diabetes mellitus status was ascertained through three complementary approaches: self-reported physician diagnosis, current utilization of insulin or oral hypoglycemic agents, or fulfillment of biochemical thresholds [fasting plasma glucose (FPG) ≥ 7.0 mmol/L, glycosylated hemoglobin (HbA1c) ≥ 6.5%, or 2-h postprandial glucose ≥ 11.0 mmol/L]. Hypertension was characterized by meeting either of two conditions: (1) documented systolic blood pressure ≥ 140 mmHg or diastolic pressure ≥ 90 mmHg; OR (2) a prior clinical diagnosis of hypertension or active use of antihypertensive medications.
Laboratory assessment
Standardized clinical records provided an extensive array of biochemical indices, including complete blood count parameters, C-reactive protein (CRP) levels, glucose metabolism markers (FPG and HbA1c), hepatic transaminases [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)], serum lipid profiles (total cholesterol and triglycerides), and serum creatinine concentrations. All laboratory assays were performed in accordance with rigorously controlled measurement protocols.
Statistical analysis
Categorical variables were presented as frequencies (percentages), whereas continuous variables were reported as mean values with standard deviations. Group comparisons for normally distributed variables were conducted using independent-samples t-tests, non-normally distributed parameters were analyzed using Mann-Whitney U-tests, and categorical data were assessed using Pearson’s chi-squared tests. The association between H. pylori seropositivity and MAFLD risk was investigated using logistic regression analysis. Kaplan-Meier curves were used to evaluate survival probability differences between H. pylori antibody-positive and antibody-negative groups. The relationship between H. pylori seropositivity and all-cause mortality was examined using the Cox proportional hazards regression model.
To address potential multicollinearity among the variables, we first assessed pairwise collinearity using the variance inflation factor and correlation coefficients. Strong multicollinearity was detected among the following variable pairs: BMI and waist circumference; FPG and HbA1c; ALT and AST; and serum cholesterol and triglycerides. Based on this criterion, waist, HbA1c, AST, and triglycerides were selected over their collinear counterparts (BMI, FPG, ALT, serum cholesterol, respectively) for inclusion in the multivariate Cox proportional hazards regression model. A two-tailed significance threshold of P < 0.05 was applied for all statistical tests. Data analyses were conducted using the R software version 4.3.3 (www.r-project.org). The survival analysis was performed with the R package “survival” employing the Kaplan-Meier method.
RESULTS
Baseline characteristics
A total of 5,946 participants who completed both ultrasound examination and H. pylori antibody testing were initially screened for this study [Figure 1]. Following the exclusion of 413 participants lacking follow-up data and 460 with missing baseline clinical characteristics, 5,073 individuals were included in the final analytical cohort. Of these, 2,630 (51.8%) were male, with a mean age of 43.3 ± 15.9 years. Hypertension and diabetes were present in 2,378 (46.9%) and 685 (13.5%) participants, respectively. A total of 2,394 (47.2%) participants were seropositive for H. pylori antibodies. Among the population, 1,610 cases met the MAFLD diagnostic criteria, with a prevalence of 31.7%.
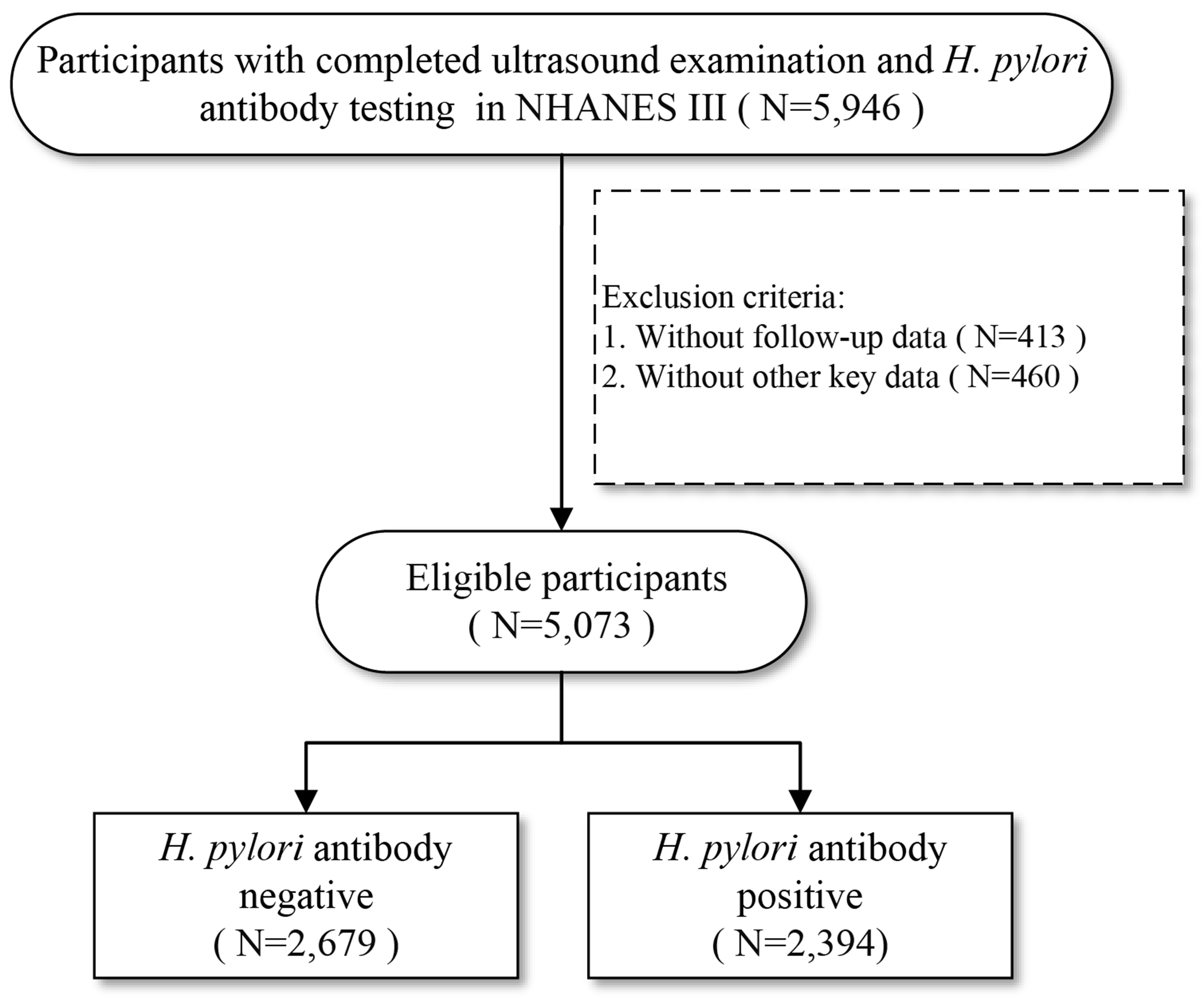
Figure 1. The flow chart of case selection. H. pylori: Helicobacter pylori; NHANES III: the Third National Health and Nutrition Examination Survey.
Comparison by H. pylori serological status
Based on H. pylori antibody test results, the participants were categorized as seropositive or seronegative. Comparative analysis of baseline characteristics [Table 1] revealed that the seropositive group was significantly older (46.2 ± 16.0 years vs. 40.8 ± 15.4 years; P < 0.001) and had a greater percentage of male participants (55.3% vs. 48.8%; P < 0.001). Furthermore, the seropositive group exhibited a higher prevalence of diabetes, hypertension, and markers of metabolic dysregulation, including elevated BMI, waist circumference, FPG, HbA1c, and serum cholesterol and triglycerides. Indicators of liver injury (ALT and AST) were also elevated more frequently in the seropositive group. Notably, the prevalence of MAFLD was significantly higher among seropositive individuals than among their seronegative counterparts (36.6% vs. 27.4%).
Baseline demographic and clinical characteristics of the study population according to H. pylori serological status
| Variables | H. pylori antibody | P-value | ||
| Total | Negative | Positive | ||
| N | 5,073 | 2,679 | 2,394 | |
| All-cause mortality, n (%) | 1,891 (37.3) | 849 (31.7) | 1,042 (43.5) | < 0.001 |
| Follow-up time (years) | 28.8 (21.7, 29.9) | 29.1 (25.5, 30.1) | 28.6 (18.7, 29.7) | < 0.001 |
| Race, n (%) | < 0.001 | |||
| Non-Hispanic white | 2,026 (39.9) | 1,421 (53.0) | 605 (25.3) | |
| Non-Hispanic black | 1,318 (26.0) | 592 (22.1) | 726 (30.3) | |
| Mexican-American | 1,545 (30.5) | 578 (21.6) | 967 (40.4) | |
| Other | 184 (3.6) | 88 (3.3) | 96 (4.0) | |
| Male (%) | 2,630 (51.8) | 1,307 (48.8) | 1,323 (55.3) | < 0.001 |
| Age (years) | 43.3 ± 15.9 | 40.8 ± 15.4 | 46.2 ± 16.0 | < 0.001 |
| Type 2 diabetes, n (%) | 685 (13.5) | 278 (10.4) | 407 (17.0) | < 0.001 |
| Hypertension, n (%) | 2,378 (46.9) | 1,131 (42.2) | 1,247 (52.1) | < 0.001 |
| BMI (kg/m2) | 26.8 ± 5.5 | 26.4 ± 5.5 | 27.3 ± 5.5 | < 0.001 |
| Waist (cm) | 92.6 ± 14.3 | 91.3 ± 14.6 | 94 ± 13.8 | < 0.001 |
| Platelets (× 109/L) | 284.4 ± 71.0 | 283.7 ± 69.6 | 285.1 ± 72.6 | 0.495 |
| CRP (mg/dL) | 0.2 (0.2, 0.3) | 0.2 (0.2, 0.3) | 0.2 (0.2, 0.4) | < 0.001 |
| FPG (mmol/L) | 5.4 ± 2.0 | 5.2 ± 1.7 | 5.6 ± 2.2 | < 0.001 |
| HbA1c (%) | 5.4 ± 1.1 | 5.3 ± 1.0 | 5.6 ± 1.2 | < 0.001 |
| Cholesterol (mmol/L) | 5.3 ± 1.1 | 5.2 ± 1.1 | 5.4 ± 1.2 | < 0.001 |
| Triglyceride (mmol/L) | 1.6 ± 1.4 | 1.5 ± 1.4 | 1.7 ± 1.3 | < 0.001 |
| AST (U/L) | 19 (16, 24) | 19 (16, 23) | 20 (17, 25) | < 0.001 |
| ALT (U/L) | 13 (10, 19) | 13 (10, 19) | 14 (10, 20) | < 0.001 |
| Creatinine (μmol/L) | 93.7 ± 25.3 | 92.9 ± 22.7 | 94.7 ± 27.8 | 0.012 |
| MAFLD | 1610 (31.7) | 733 (27.4) | 877 (36.6) | < 0.001 |
H. pylori association with MAFLD
As shown in Table 2, univariate logistic regression revealed that H. pylori seropositivity was a significant risk factor for MAFLD [unadjusted OR = 1.535, 95% confidence interval (CI): 1.363-1.729, P < 0.001]. This association persisted in multivariable analyses accounting for prespecified confounders. In Model 1 (adjusted for sex, age, race, diabetes, and hypertension), the OR was 1.422 (95%CI: 1.260-1.605, P < 0.001). After further adjustment for BMI, Platelets (PLT), CRP, FPG, serum cholesterol, ALT, and creatinine levels (Model 2), the OR remained significant at 1.282 (95%CI: 1.126-1.459, P < 0.001). These results confirm that H. pylori seropositivity is an independent predictor of MAFLD risk.
Logistic regression analysis of H. pylori seropositivity and MAFLD risk
| Model | OR (95%CI) | P-value |
| Crude | 1.535 (1.363-1.729) | < 0.001 |
| Model 1 | 1.422 (1.260-1.605) | < 0.001 |
| Model 2 | 1.282 (1.126-1.459) | < 0.001 |
All-cause mortality grouped by H. pylori antibody
With a median follow-up of 28.8 years (interquartile range: 21.7-29.9), 1,891 deaths occurred within the cohort, resulting in an overall cumulative mortality rate of 37.3%. As shown in Table 1, individuals seropositive for H. pylori had significantly higher mortality rates than seronegative individuals (43.5% vs. 31.7%, P < 0.001). A significant difference in survival probability between the H. pylori-positive and negative groups was demonstrated by Kaplan-Meier analysis (log-rank P < 0.001; Figure 2A). This survival disadvantage associated with H. pylori seropositivity became apparent within the initial ten years of follow-up and continued to increase over time. By the 30-year mark, the absolute difference in survival was 11.8% (seropositive: 56.5% vs. seronegative: 68.3%). Consistently, the Kaplan-Meier curves showed significantly greater survival probabilities in H. pylori-negative individuals, a pattern evident in both the non-MAFLD [Figure 2B] and MAFLD [Figure 2C] subgroups (log-rank P < 0.001 for each).
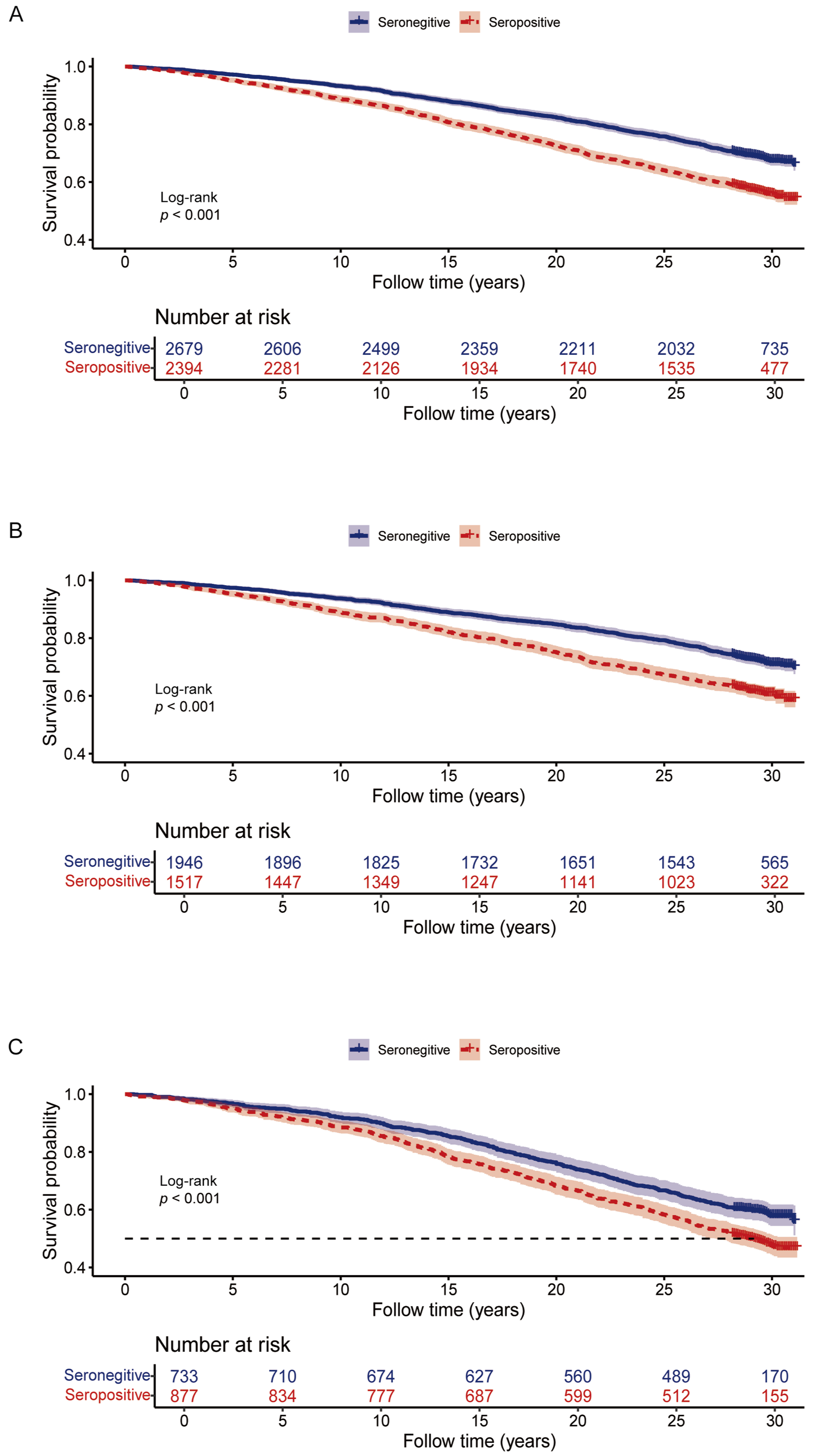
Figure 2. Kaplan-Meier analysis comparing H. pylori-seropositive and seronegative participants. (A) Total population; (B) non-MAFLD group; and (C) MAFLD group. Log-rank test P-values are shown. H. pylori: Helicobacter pylori; MAFLD: metabolic dysfunction-associated fatty liver disease.
Cox regression analysis
To assess the relationship between H. pylori seropositivity and all-cause mortality within the entire cohort, Cox proportional hazards regression analysis was conducted. The findings are presented in Table 3 and Figure 3. The initial unadjusted analysis indicated a significant association between seropositivity for
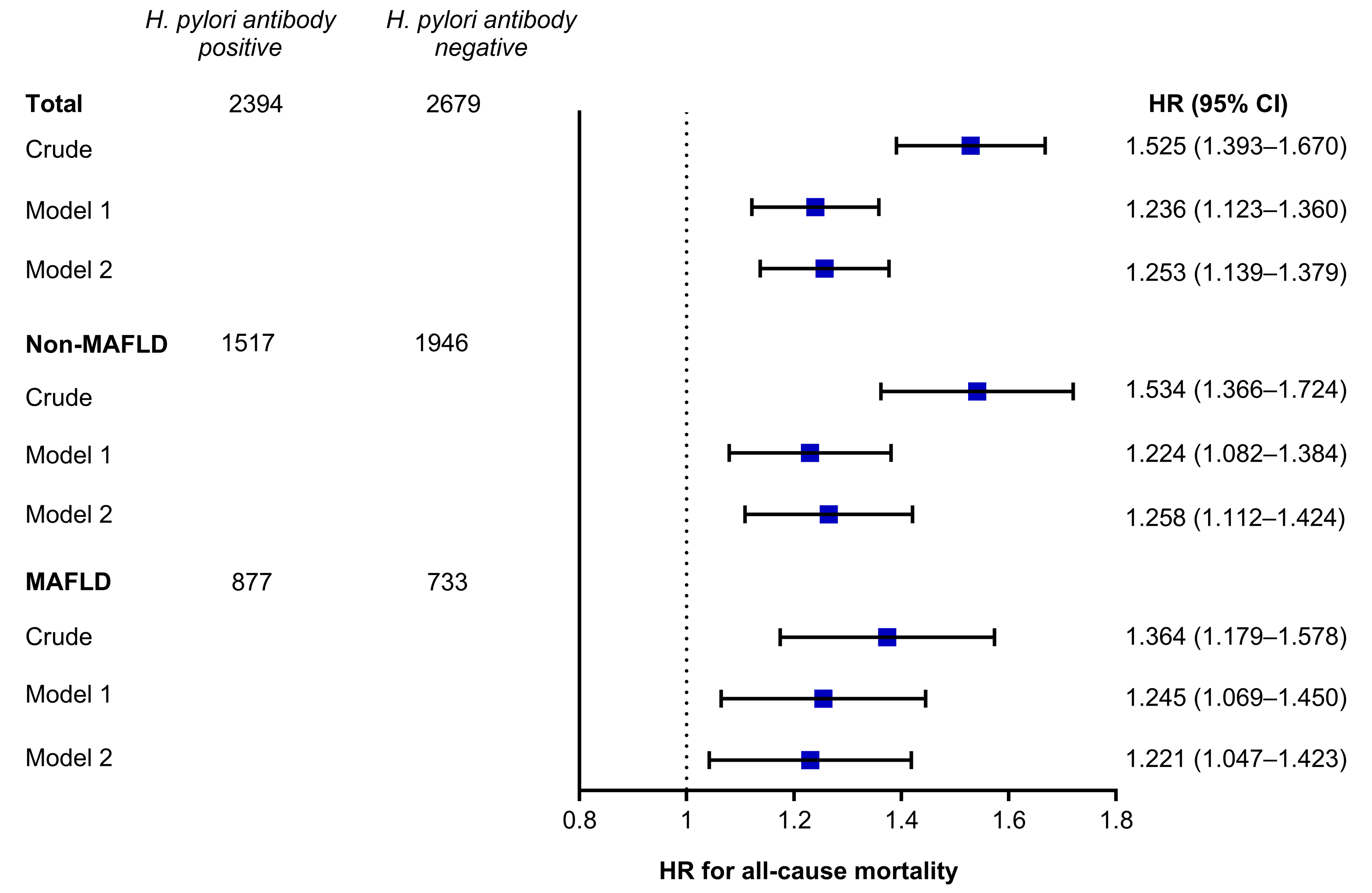
Figure 3. Forest plot of estimated HRs for mortality according to H. pylori status based on Cox regression analysis. HRs: Hazard ratios; H. pylori: Helicobacter pylori; CI: confidence interval; MAFLD: metabolic dysfunction-associated fatty liver disease.
Cox regression analysis of the association between H. pylori seropositivity and all-cause mortality
| Model | Total | non-MAFLD | MAFLD | |||
| HR (95%CI) | P-value | HR (95%CI) | P-value | HR (95%CI) | P-value | |
| Crude | 1.525 (1.393-1.670) | < 0.001 | 1.534 (1.366-1.724) | < 0.001 | 1.364 (1.179-1.578) | < 0.001 |
| Model 1 | 1.236 (1.123-1.360) | < 0.001 | 1.224 (1.082-1.384) | 0.001 | 1.245 (1.069-1.450) | 0.005 |
| Model 2 | 1.253 (1.139-1.379) | < 0.001 | 1.258 (1.112-1.424) | < 0.001 | 1.221 (1.047-1.423) | 0.011 |
The results are presented for the total population, the non-MAFLD group, and the MAFLD group across three adjustment models: crude (unadjusted), Model 1 (adjusted for sex, age, race, diabetes, and hypertension), and Model 2 (additionally adjusted for BMI, PLT, CRP, FPG, serum cholesterol, ALT, and creatinine levels).
DISCUSSION
The present study demonstrated a notable association between H. pylori seropositivity and MAFLD, along with an elevated risk of all-cause mortality, independent of conventional metabolic and inflammatory confounders. These findings add to the expanding body of literature connecting H. pylori to systemic health outcomes beyond its recognized involvement in gastrointestinal disorders.
Our results revealed a 36.6% prevalence of MAFLD in H. pylori-seropositive individuals, significantly higher than the 27.4% prevalence observed in their seronegative counterparts. This association persisted after adjusting for metabolic factors and inflammatory markers, suggesting that H. pylori may exacerbate hepatic lipid accumulation through mechanisms independent of conventional metabolic derangements. Several meta-analyses have demonstrated that H. pylori infection is associated with an elevated risk of prevalent MAFLD, with odds ratios (OR) ranging from 1.20 to 1.27[14,20,21]. A cross-sectional study has reported a positive association between H. pylori seropositivity and triglyceride levels (OR = 1.231)[22]. In a case-control study, H. pylori-infected individuals exhibited elevated low-density lipoprotein cholesterol and reduced high-density lipoprotein cholesterol concentrations[23]. The prevalence of H. pylori infection was significantly higher among participants with diabetes than in those without diabetes[24]. Population-based studies have indicated that H. pylori infection may exacerbate insulin resistance, leading to elevated lipid and glucose levels and subsequently triggering metabolic abnormalities[25], thereby increasing the risk of MAFLD. Experimental animal studies have shown that H. pylori aggravates MAFLD progression by modulating hepatic lipid metabolism through its virulence factor, the cytotoxin-associated gene A (CagA) protein[26]. Another study revealed dynamic alterations in the gut microbiota consistent with H. pylori-induced metabolic phenotype changes[27]. Therefore, the mechanisms underlying H. pylori-induced metabolic disturbances remain complex and warrant further investigations to validate these preliminary findings.
Even after rigorous adjustment for metabolic and inflammatory variables, H. pylori seropositivity was associated with an 11.8 percentage point higher all-cause mortality rate. This suggests that H. pylori infection poses a systemic health threat. This survival disadvantage emerged early (within 10 years) and widened over time, which is consistent with the cumulative effects of chronic inflammation and microvascular damage. Notably, the mortality gap persisted in both the MAFLD and non-MAFLD subgroups, suggesting that
In light of the potential association between H. pylori seropositivity and increased MAFLD prevalence, researchers have begun preliminary studies to examine whether H. pylori affects MAFLD. Despite these efforts, the body of literature remains sparse, and the findings are inconclusive. Yu et al. demonstrated that the eradication of H. pylori could further ameliorate metabolic indices and reduce the degree of hepatic steatosis in patients with MAFLD[29]. Conversely, a separate randomized, open-label clinical trial indicated that the eradication of H. pylori might not significantly influence liver fat content, liver function tests, blood lipid profiles, or insulin resistance in patients with MAFLD[30]. Considering the practicality and cost-effectiveness of eradicating H. pylori, further research is necessary to determine whether targeted treatment can mitigate MAFLD-related complications and enhance survival.
A key strength of this study is its large, population-based cohort, combined with long-term follow-up (median 28.8 years), enabling a robust assessment of temporal trends in mortality. Additionally, adjustment for multiple confounders (e.g., BMI, CRP, and lipid profiles) strengthens the validity of our conclusions. Nevertheless, several limitations should be noted. First, the observational design precludes causal inferences, and residual confounding by unmeasured factors (e.g., smoking, diet, socioeconomic status) cannot be excluded. Second, H. pylori seropositivity reflects past exposure rather than active infection, and data on eradication therapy were unavailable, limiting insights into reversibility. Third, the lack of direct measurements of liver histology or advanced fibrosis precludes detailed mechanistic conclusions. Future studies should prioritize prospective designs, incorporate H. pylori DNA detection or the 13C-urea breath test to confirm active infection[31], and explore the mediators[32] (e.g., interleukin-6 and adiponectin) linking H. pylori to metabolic and hepatic outcomes.
Conclusions
In summary, this population-based epidemiological follow-up study demonstrated a significant correlation between H. pylori seropositivity and an increased risk of MAFLD and all-cause mortality. These findings highlight the enduring public health impact of H. pylori as a chronic bacterial infection, indicating the need for further research to ascertain whether eradication of H. pylori could reduce the risk of MAFLD and mortality in the general population.
DECLARATIONS
Acknowledgments
The Graphical Abstract was created in BioRender. Fan, Q. (2026) https://BioRender.com/2ecggp1.
Authors’ contributions
Conceived the study design, supervised the project, and critically revised the manuscript for important intellectual content: Huang J
Performed the statistical analysis and was responsible for manuscript preparation: Fan Q
Conducted the primary data analysis and visualization: Chen Y
Contributed to the clinical interpretation of the findings and assisted in the literature review: Liu J, Gao L
Availability of data and materials
Publicly available datasets were analyzed in this study. The raw data used in the article are available on the National Health and Nutrition Examination Survey website (https://wwwn.cdc.gov/nchs/nhanes/Default.aspx).
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tools Gemini 3 Pro and DeepSeek-V3.2 were used solely for language editing. The tools did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
This study was supported by the Joint Funds for the Innovation of Science and Technology, Fujian Province (No. 2024Y9131).
Conflicts of interest
Huang J is a Junior Editorial Board Member of Hepatoma Research. Huang J was not involved in any part of the editorial process for this manuscript, including reviewer selection, manuscript handling, or decision-making. The other authors declare that they have no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Li Y, Choi H, Leung K, Jiang F, Graham DY, Leung WK. Global prevalence of Helicobacter pylori infection between 1980 and 2022: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2023;8:553-64.
2. Duan Y, Xu Y, Dou Y, Xu D. Helicobacter pylori and gastric cancer: mechanisms and new perspectives. J Hematol Oncol. 2025;18:10.
3. Tsay FW, Hsu PI. H. pylori infection and extra-gastroduodenal diseases. J Biomed Sci. 2018;25:65.
4. Yaslianifard S, Sameni F, Kazemi K, et al. Beyond the gut: a comprehensive meta-analysis on Helicobacter pylori infection and cardiovascular complications. Ann Clin Microbiol Antimicrob. 2025;24:18.
5. Penaflorida JLGR, Requesto JRU, Romero KYB, et al. Association between Helicobacter pylori and hepatobiliary cancer: a meta-analysis and systematic review. Asian Pac J Cancer Prev. 2024;25:3363-70.
6. Fabbri N, Greco S, Pesce A, Virgilio F, Romeo D, Feo CV. Role of Helicobacter pylori infection and the risk of cholelithiasis. World J Gastroenterol. 2025;31:102024.
7. Lazarus JV, Colombo M, Cortez-Pinto H, et al. NAFLD - sounding the alarm on a silent epidemic. Nat Rev Gastroenterol Hepatol. 2020;17:377-9.
8. Riazi K, Azhari H, Charette JH, et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7:851-61.
9. Estes C, Razavi H, Loomba R, Younossi Z, Sanyal AJ. Modeling the epidemic of nonalcoholic fatty liver disease demonstrates an exponential increase in burden of disease. Hepatology. 2018;67:123-33.
10. Guo W, Ge X, Lu J, et al. Diet and risk of non-alcoholic fatty liver disease, cirrhosis, and liver cancer: a large prospective cohort study in UK biobank. Nutrients. 2022;14:5335.
11. Mostafa AM, Pan Z, Yu ML, Örmeci N, Fouad Y, Eslam M. MAFLD: a comprehensive review of the link between metabolic dysfunction and cardiovascular risk. Hepat Med. 2025;17:75-90.
12. Yuan X, Wang X, Wu S, et al. Associations between metabolic dysfunction-associated fatty liver disease and extrahepatic cancers: a cohort in China. Hepatobiliary Surg Nutr. 2023;12:671-81.
13. Dong TS, Luu K, Lagishetty V, et al. Gut microbiome profiles associated with steatosis severity in metabolic associated fatty liver disease. Hepatoma Res. 2021;7:37.
14. Heydari K, Yousefi M, Alizadeh-Navaei R, et al. Helicobacter pylori infection and non-alcoholic fatty liver disease: a systematic review and meta-analysis. Turk J Gastroenterol. 2022;33:171-81.
15. Gulati A, Roytman M, Lin J, et al. Association between Helicobacter pylori infection, MASLD, and liver fibrosis in patients with severe obesity: a single-center experience. Surg Endosc. 2024;38:6873-9.
16. Liu Y, Xu H, Zhao Z, Dong Y, Wang X, Niu J. No evidence for a causal link between Helicobacter pylori infection and nonalcoholic fatty liver disease: A bidirectional Mendelian randomization study. Front Microbiol. 2022;13:1018322.
17. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202-9.
18. Centers for Disease Control and Prevention. NHANES 1999-2000 Laboratory Methods. Available from https://wwwn.cdc.gov/nchs/nhanes/continuousnhanes/labmethods.aspx?BeginYear=1999. [accessed 4 June 2026].
19. Centers for Disease Control and Prevention. Questionnaires, Datasets, and Related Documentation-NHANES III. Available from https://wwwn.cdc.gov/nchs/nhanes/nhanes3/datafiles.aspx. [accessed 4 June 2026].
20. Wijarnpreecha K, Thongprayoon C, Panjawatanan P, Manatsathit W, Jaruvongvanich V, Ungprasert P. Helicobacter pylori and risk of nonalcoholic fatty liver disease: a systematic review and meta-analysis. J Clin Gastroenterol. 2018;52:386-91.
21. Mantovani A, Turino T, Altomari A, et al. Association between Helicobacter pylori infection and risk of nonalcoholic fatty liver disease: an updated meta-analysis. Metabolism. 2019;96:56-65.
22. Xie J, Wang J, Zeng R, Xie Y. Association between Helicobacter pylori infection and triglyceride levels: a nested cross-sectional study. Front Endocrinol. 2023;14:1220347.
23. Zhao MM, Krebs J, Cao X, et al. Helicobacter pylori infection as a risk factor for serum bilirubin change and less favourable lipid profiles: a hospital-based health examination survey. BMC Infect Dis. 2019;19:157.
24. Mansori K, Dehghanbanadaki H, Naderpour S, Rashti R, Moghaddam AB, Moradi Y. A systematic review and meta-analysis of the prevalence of Helicobacter pylori in patients with diabetes. Diabetes Metab Syndr. 2020;14:601-7.
25. Polyzos SA, Kountouras J, Zavos C, Deretzi G. The association between Helicobacter pylori infection and insulin resistance: a systematic review. Helicobacter. 2011;16:79-88.
26. Chen X, Peng R, Peng D, Liu D, Li R. Helicobacter pylori infection exacerbates metabolic dysfunction-associated steatotic liver disease through lipid metabolic pathways: a transcriptomic study. J Transl Med. 2024;22:701.
27. He C, Yang Z, Cheng D, et al. Helicobacter pylori infection aggravates diet-induced insulin resistance in association with gut microbiota of mice. EBioMedicine. 2016;12:247-54.
28. Candelli M, Franza L, Cianci R, et al. The interplay between Helicobacter pylori and gut microbiota in non-gastrointestinal disorders: a special focus on atherosclerosis. Int J Mol Sci. 2023;24:17520.
29. Yu YY, Tong YL, Wu LY, Yu XY. Helicobacter pylori infection eradication for nonalcoholic fatty liver disease: a randomized controlled trial. Sci Rep. 2022;12:19530.
30. Jamali R, Mofid A, Vahedi H, Farzaneh R, Dowlatshahi S. The effect of Helicobacter pylori eradication on liver fat content in subjects with non-alcoholic Fatty liver disease: a randomized open-label clinical trial. Hepat Mon. 2013;13:e14679.
31. Kamboj AK, Cotter TG, Oxentenko AS. Helicobacter pylori: the past, present, and future in management. Mayo Clin Proc. 2017;92:599-604.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].