


From algorithm to dialogue: interpreting the 2026 BCLC-CUSE strategy for HCC care
 0
0 
HEPATOCELLULAR CARCINOMA: A GROWING EPIDEMIOLOGICAL AND CLINICAL CONCERN
Historically linked with viral hepatitis and alcohol consumption, hepatocellular carcinoma (HCC), the most common form of primary liver cancer (PLC), is increasingly recognized as a disorder attributable to obesity and type 2 diabetes[1,2]. In 2021, high body mass index (BMI) and/or high fasting plasma glucose were linked to an estimated 59,970 deaths and 1,540,437 disability-adjusted life years (DALYs) from PLC worldwide. Age-standardized death and DALY rates were 0.70 and 17.64 per 100,000 person-years. Liver cancer from metabolic risks has steadily increased since 1990, with high BMI as the main factor. The greatest burden was in high sociodemographic index (SDI) countries, while low-middle SDI regions saw the fastest growth. Men typically experience higher disease burdens than women[2].
It is a fact that HCC is one of the deadliest cancers and is characterized by profound metabolic reprogramming, increased de novo lipid synthesis, and a complex suppressive immune tumor microenvironment[3]. These mechanisms are closely linked with metabolic dysfunction-associated steatotic liver disease (MASLD), which has become the most prevalent chronic liver disease worldwide and an increasingly important cause of HCC. MASLD-associated tumors often display immune-cell exhaustion and tumor-associated macrophage accumulation, potentially contributing to reduced responsiveness to immune checkpoint inhibitor therapies in some patients[3].
Over the past decade, the therapeutic landscape of HCC has changed substantially, particularly with the introduction of immune-based systemic therapies. While sorafenib was long the only systemic option for advanced disease, several immune checkpoint inhibitor combinations have now demonstrated improved survival and have become preferred first-line treatments [Figure 1].
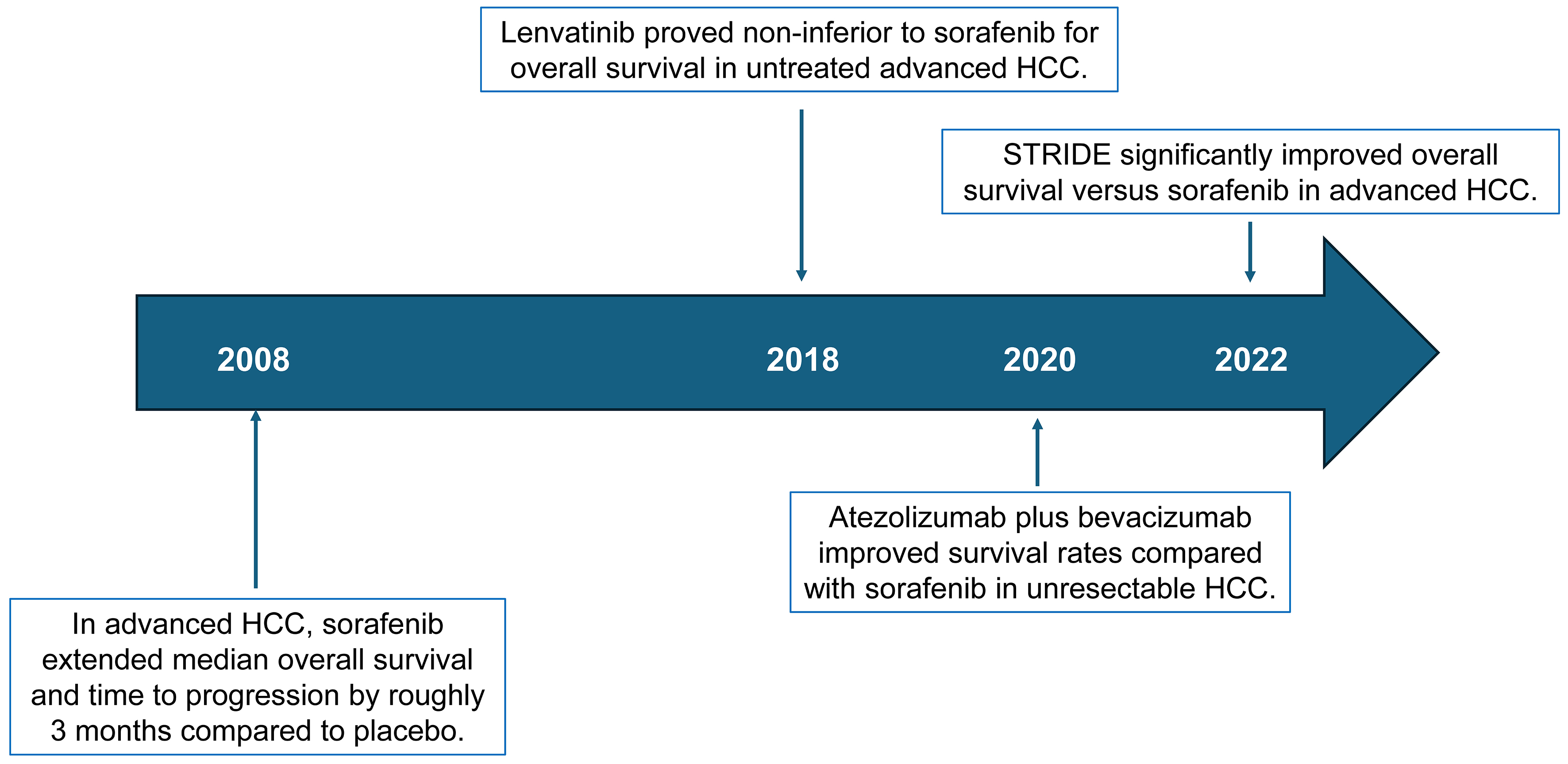
Figure 1. Main advances in the treatment of hepatocellular carcinoma. The graphical illustration highlights some key breakthroughs in the medical treatment of advanced HCC, based on seminal studies by Llovet et al.[4], Kudo et al.[5], Finn et al.[6], and Abou-Alfa et al.[7]. HCC: Hepatocellular carcinoma; STRIDE: Single Tremelimbumab Regular Interval Durvalumab.
Regimens such as atezolizumab-bevacizumab have shown clinically meaningful benefits compared with earlier tyrosine kinase inhibitor monotherapies, reflecting a shift toward immunotherapy-based strategies. In parallel, advances in locoregional treatments, including improved techniques for thermal ablation, transarterial therapies, and stereotactic radiotherapy, have expanded the therapeutic armamentarium for selected patients across different disease stages. Moreover, the dual-immunotherapy regimen Single Tremelimbumab Regular Interval Durvalumab (STRIDE) has become an attractive therapeutic option as a first-line treatment for adults with advanced or unresectable HCC.
A CONSERVATIVE STAGING UPDATE WITH CLEARER PROGNOSTIC ANCHORING
For more than two decades, the Barcelona Clinic Liver Cancer (BCLC) staging system has served as a central framework for the prognosis assessment and treatment allocation of HCC, which appears frequently in patients with cirrhosis[8-10]. The recently published 2026 update[11] preserves the established five-stage structure but reframes BCLC less as a rigid algorithm and more as a starting point for structured clinical discussion as therapeutic options continue to expand.
The revised framework links each stage to evidence-based first-line strategies while providing clearer prognostic benchmarks. Expected median overall survival with optimal therapy exceeds five years for BCLC-0/A disease, more than 2.5 years for BCLC-B, approximately two years for BCLC-C, and less than one year for BCLC-D. The update also reinforces the prognostic role of the albumin-bilirubin (ALBI) score as a complement to the Child-Pugh classification and highlights alpha-fetoprotein (AFP) as an important prognostic marker and determinant in transplant eligibility.
The 2026 update consolidates, rather than replaces, prior prognostic refinements. ALBI grading is endorsed as a complementary measure of hepatic reserve to Child-Pugh, particularly for differentiating compensated from decompensated cirrhosis. AFP is reaffirmed as a negative prognostic marker and transplant criterion; levels ≥ 1,000 ng/mL indicate high recurrence risk and usually preclude transplantation regardless of tumor burden.
One significant technical refinement is the revised definition of “multifocal” intermediate-stage disease, now defined as either having more than three nodules or up to three nodules with at least one being larger than 3 cm. This clarification aims to simplify the distinction between BCLC-A and BCLC-B, which has previously complicated trial design and treatment decisions in clinical practice.
CUSE: NAMING THE UNCERTAINTY WE ALL LIVE WITH
A central innovation of the 2026 update is the explicit integration of the CUSE framework (Complexity, Uncertainty, Subjectivity, Emotion) into clinical decision-making[11]. The authors recognize that many therapeutic decisions in HCC occur in situations where randomized evidence is incomplete or not directly comparable. CUSE therefore proposes a structured and iterative approach in which clinicians define care goals, assess clinical and social context, evaluate the strength of available evidence, deliberate within a multidisciplinary team, and document shared decisions with patients[11]. Importantly, CUSE deliberately shifts language from “best” to “optimal” option when direct comparative evidence is lacking, an apparently semantic change that in practice legitimizes acknowledging doubt at the bedside.
The authors also introduce pragmatic decision thresholds, GO (clear goal, robust safety evidence, favorable benefit-risk, adequate hepatic reserve and performance status, and assured deliver-ability), CONSIDER (marginal eligibility or modifiable risks needing optimization, including prehabilitation strategies to enhance physical reserve, information gaps to address, or suitability for an approved clinical trial), and NO-GO (high decompensation risk, absolute contraindications, uncontrolled comorbidity, non-deliverable care (logistics, access, or affordability constraints), or absence of robust safety evidence.
Outside approved trials, these options should be avoided, favoring best supportive care or stage-appropriate alternatives. Decision-making should integrate evidence strength, hepatic reserve, performance status, toxicity risk, and feasibility, particularly for off-label or regionally restricted interventions and for settings in which progression-free survial (PFS) gains do not clearly translate into overall survial (OS) benefit, as reported for several transarterial chemoembolization (TACE)-based combinations and intermediate-stage immunotherapy trials. As such, the forthcoming BCLC-CUSE. AI tool may support tumor boards by integrating trial evidence and case-specific factors, provided data sources, limitations, and clinical accountability remain explicit.
LOCOREGIONAL THERAPY: EXPANDING OPTIONS WITHOUT OVERSTATING EVIDENCE
In early-stage (BCLC-0/A) disease, the update includes a broadening ablative toolbox while avoiding the creation of a pseudo-hierarchy not supported by head-to-head trials. Percutaneous thermal ablation (especially microwave) remains the preferred alternative to surgery for single tumors ≤ 3-4 cm. This is supported by randomized controlled trials (RCTs) and long-term cohort data. Transarterial radioembolization (TARE) and external-beam radiotherapy (EBRT), including stereotactic body radiotherapy (SBRT), are now explicitly recognized as ablative-intent options in selected BCLC-0/A patients, based on prospective and pooled data showing multi-year OS similar to that achieved with more established modalities (e.g., surgery or thermal ablation).
The authors rightly stress heterogeneity and selection bias in these datasets and place TARE/EBRT within a CUSE-guided framework rather than as default first-line replacements. This is a welcome corrective to the sometimes overly enthusiastic interpretation of small series or single-arm studies, particularly when advocating resource-intense technologies.
In BCLC-B, TACE retains its status as the standard of care in well-selected patients, with the update carefully dissecting the nuanced and sometimes contradictory literature on drug-eluting beads vs. bland embolization vs. TARE vs. EBRT. The authors avoid over-interpreting indirect comparisons and underline that, in compensated patients with suitable vascular anatomy, TACE still offers the strongest survival evidence from randomized trials. TARE and EBRT are framed as reasonable options when TACE is not feasible or has failed, but not as proven first-line alternatives based on OS.
SYSTEMIC THERAPY AND SEQUENCES: INSTITUTIONALIZING HUMILITY
For advanced-stage (BCLC-C) disease, the 2026 strategy aligns with contemporary practice by recommending immune-based combinations, such as atezolizumab-bevacizumab, tremelimumab-durvalumab, ipilimumab-nivolumab, or camrelizumab-rivoceranib, as preferred first-line options over sorafenib. However, Reig and colleagues deliberately refrain from ranking these regimens, citing the absence of head-to-head trials and the confounding introduced by differing eligibility criteria, regional recruitment, and proportions of non-C BCLC stages in pivotal studies[11]. Immune checkpoint inhibitors’ efficacy varies by HCC etiology, with stronger responses generally reported in virus-related HCC and attenuated activity in non-viral tumors, particularly those associated with metabolic dysfunction-associated steatohepatitis (MASH).
Perhaps more importantly, the authors explicitly acknowledge that validated second-line pathways exist only for sorafenib-pretreated patients, and that sequencing after immunotherapy is supported largely by phase II trials and real-world cohorts. In these situations, CUSE is again invoked to structure choices around preservation of liver function, tolerability, access to trials, and patient preferences, rather than around tenuous cross-trial comparisons.
The update is also refreshingly cautious regarding “conversion” and “systemic treatment prior to liver transplant”. Major tumor regressions during immunotherapy and/or combination strategies are recognized as a distinct clinical state called “treatable tumor regression”. In this stage, a tumor that was initially considered inoperable or untreatable becomes treatable (usually via surgery) after a positive response to treatment, such as chemotherapy or radiation. However, the authors classify all post-immunotherapy surgery, ablation, or transplantation as “alternative sequences” that are not yet robustly proven and should be considered temporary, case-by-case decisions.
END-STAGE DISEASE AND RECOMPENSATION: AVOIDING THERAPEUTIC OVERREACH
Finally, BCLC-D is revisited considering emerging data on cirrhosis recompensation. Although Baveno VII recompensation may reopen options such as liver transplantation (LT) or systemic therapy, Reig et al. emphasize that durable recompensation is uncommon and tumor progression remains a concern[11,12]. Thus, best supportive care remains central for most BCLC-D patients, with an expected median OS of < 12 months and emphasis on symptom control and palliative care.
WHERE DO WE GO FROM HERE?
The 2026 BCLC strategy represents less a conceptual revolution than a maturation of the framework guiding HCC management. Its key contribution lies in acknowledging evidence gaps while providing a structured method for navigating them. By integrating CUSE principles with established staging, the update emphasizes transparent reasoning, multidisciplinary discussion, and shared decision-making when determining the most appropriate treatment strategy. Importantly, the integration of the CUSE framework acknowledges that different underlying etiologies and clinical variations require tailored treatment adjustment.
Although both the 2026 BCLC strategy and the Chinese guidelines incorporate contemporary immunotherapeutic advances, they reflect distinct clinical frameworks shaped by regional epidemiology. The BCLC approach emphasizes evidence hierarchy, liver function, tumor burden, and CUSE-guided shared decision-making[11]. By contrast, the Chinese guidelines adopt a more HBV-oriented and intervention-intensive strategy, prioritizing biomarker-based screening, antiviral therapy, and multimodal locoregional approaches to broaden resectability[13].
Several research priorities emerge from this strategy: prospective evaluation of CUSE-guided decisions (including metrics of decisional quality and patient-reported outcomes); head-to-head or carefully designed comparative effectiveness studies for locoregional therapies in BCLC-0/BCLC-A/BCLC-B; robust sequencing trials after first-line immunotherapy; and systematic tracking of outcomes for “alternative sequences” such as immunotherapy-bridged LT and conversion surgery.
For clinicians and tumor boards, the message is clear: BCLC remains the starting point, but CUSE reminds us that navigation is a human, iterative process. The effectiveness of the 2026 strategy will rely not only on forthcoming data but also on our commitment to clearly acknowledging uncertainty and collaboratively sharing responsibility for making “optimal decisions” with patients, families, and colleagues, rather than pursuing “the best options”.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the commentary, as well as performed literature analysis and interpretation: Weiskirchen R, Lonardo A
Availability of data and materials
Not applicable.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool chatGPT (version 5.3, released 2025-08-07) was used solely for language editing. The tool did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Financial support and sponsorship
None.
Conflicts of interest
Lonardo A is an Associate Chief Editor of the journal Hepatoma Research. He was not involved in any part of the editorial process for this manuscript, including reviewer selection, manuscript handling, or decision-making. Weiskirchen R declares that there are no conflicts of interest.
Ethical approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Lugari S, Baldelli E, Lonardo A. Metabolic primary liver cancer in adults: risk factors and pathogenic mechanisms. Metab Target Organ Damage. 2023;3:5.
2. Wu C, Targher G, Byrne CD, et al. Global, regional, and national burden of primary liver cancer attributable to metabolic risks: an analysis of the Global Burden of Disease Study 1990-2021. Am J Gastroenterol. 2025;120:2280-90.
3. Weiskirchen R, Lonardo A. Obesity, metabolic dysfunction-associated steatotic liver disease and hepatocellular carcinoma: how molecular changes impact cellular functions. BIOCELL. 2026;50:1-10.
4. Llovet JM, Ricci S, Mazzaferro V, et al. ; SHARP Investigators Study Group. Sorafenib in advanced hepatocellular carcinoma. N Engl J Med. 2008;359:378-90.
5. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised phase 3 non-inferiority trial. Lancet. 2018;391:1163-73.
6. Finn RS, Qin S, Ikeda M, et al. ; IMbrave150 Investigators. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382:1894-905.
7. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evid. 2022;1:EVIDoa2100070.
10. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on the management of hepatocellular carcinoma. J Hepatol. 2025;82:315-74.
11. Reig M, Sanduzzi-Zamparelli M, Forner A, et al. BCLC strategy for prognosis prediction and treatment recommendations: the 2026 update. J Hepatol. 2026;84:631-54.
12. de Franchis R, Bosch J, Garcia-Tsao G, Reiberger T, Ripoll C. ; Baveno VII Faculty. Baveno VII - renewing consensus in portal hypertension. J Hepatol. 2022;76:959-74.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].