


Clinical effectiveness of complete thoracoscopy vs. thoracoscopy-assisted surgery in the treatment of multiple rib fractures in non-flail chest
 0
0 Abstract
Aim: To retrospectively analyze the clinical effectiveness of complete thoracoscopy vs. thoracoscopy-assisted surgery in the treatment of multiple rib fractures in non-flail chest.
Methods: A total of 86 patients with multiple rib fractures were divided into a “Complete Thoracoscopy group” (n = 40) and a “Thoracoscopy-Assisted group” (n = 46). Perioperative clinical data, Visual Analog Scale (VAS) pain scores, and 3-month postoperative clinical effectiveness were compared between the two groups.
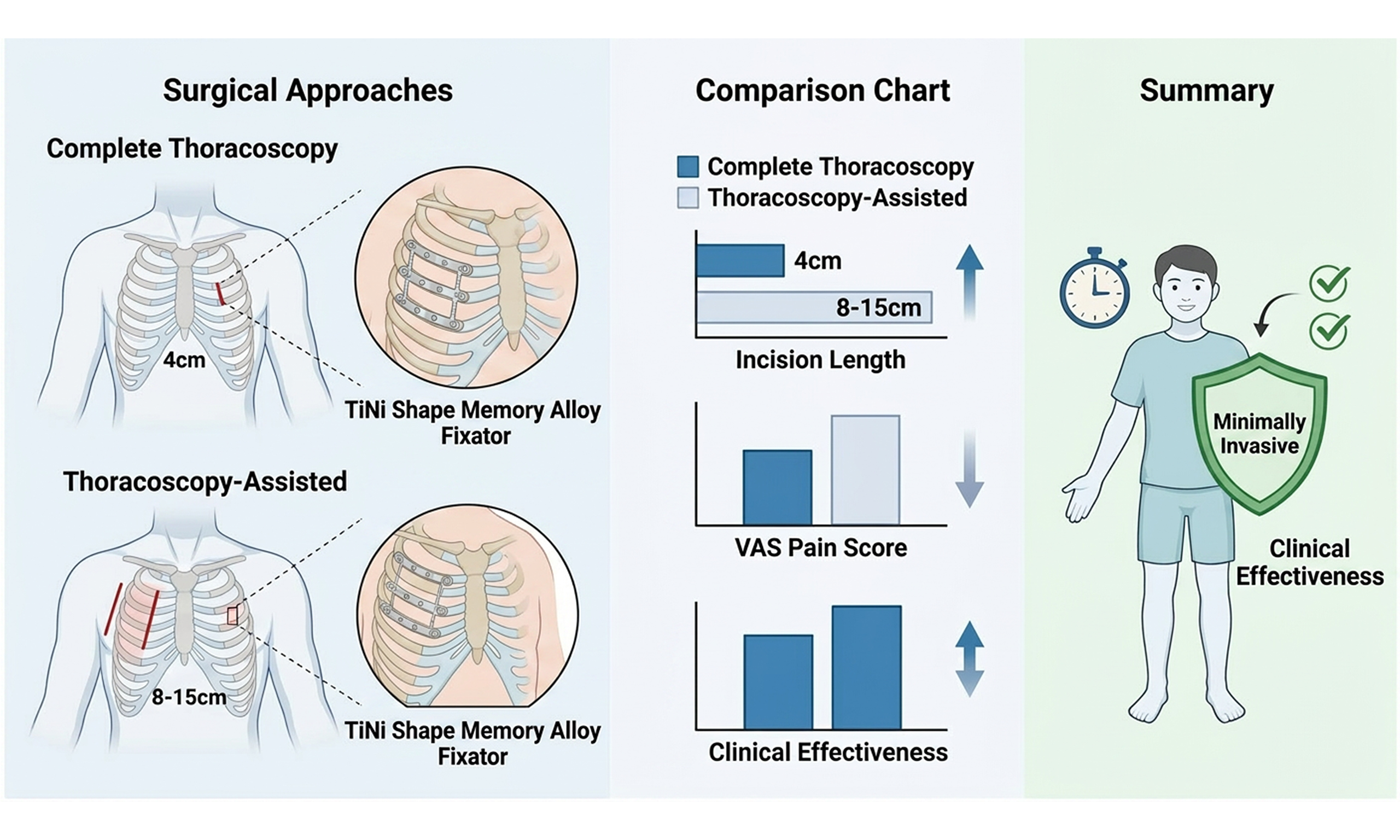
Results: There was no statistical difference between two groups of patients in basic information (P > 0.05). There was no significant difference between two groups in terms of number of rib fixation fractures during surgery, postoperative chest tube drainage volume, extubating time, postoperative hospital stays, as well as the incidence of common postoperative complications(P > 0.05). Compared with the Thoracoscopy-Assisted group, the Complete Thoracoscopy group had shorter incision length and longer surgical time (P < 0.05). On the 3rd and 7th day after surgery, the VAS scores of the Complete Thoracoscopy group were lower than those of the Thoracoscopy-Assisted group (P < 0.05). The clinical effectiveness of the Complete Thoracoscopy group was better than that of the Thoracoscopy-Assisted group at 3 months after surgery (P < 0.05).
Conclusions: Both complete thoracoscopy and thoracoscopy-assisted surgery have good surgical effects on multiple rib fractures. The complete thoracoscopy procedure has shorter incision length and less trauma, significantly reduces postoperative pain and improves clinical effectiveness. It is worth promoting and applying in clinical practice.
Keywords
INTRODUCTION
Rib fractures represent the most common type of chest trauma. Severe cases can lead to various complications such as flail chest, lung laceration, hemopneumothorax, and further progress to respiratory or circulatory failure[1,2], posing a significant threat to life. Multiple non-flail rib fractures are defined as fractures involving three or more ribs, each with a single fracture site, arranged linearly along the longitudinal axis. Due to their scattered distribution, these fractures cause segmental instability along this axis without forming a classical flail segment, yet they often result in severe pain and dyspnea[3]. Surgical stabilization of rib fractures (SSRF) has initially demonstrated satisfactory outcomes in the management of flail chest. However, its application in multiple non-flail rib fractures remains controversial. With advancements in surgical techniques, treatment concepts, and implant materials, the indications for SSRF have been gradually expanded, and corresponding guideline consensus has been established[4,5]. Conventional open reduction and internal fixation (ORIF) necessitates extensive incisions that disrupt chest-wall musculature, vasculature and intercostal nerves, predisposing to surgical-site infection, chronic neuralgia, upper-limb dysfunction and prolonged hemithorax numbness[6]. The evolution of minimally invasive surgery and endoscopic technology has facilitated increasing utilization of thoracoscopy during SSRF. Beyond enabling precise fracture localization and targeted incision planning, thoracoscopy affords simultaneous intrathoracic exploration and management of concomitant injuries[7,8]. Consequently, a hybrid strategy combining thoracoscopy with limited auxiliary incisions has become the dominant paradigm. Nevertheless, skin and soft-tissue trauma remains non-trivial, and post-operative pain continues to be problematic. In recent years, complete thoracoscopic rib fracture internal fixation has garnered increasing attention. This approach can effectively reduce incision length, minimize injury to chest wall structures, provide adequate surgical exposure, achieve satisfactory outcomes, and promote faster postoperative recovery[9]. Our institution has continuously adopted new technologies and has performed both complete thoracoscopic and thoracoscopy-assisted mini-incision surgeries for multiple non-flail rib fractures in recent years. The present retrospective study compares the clinical effectiveness of these two approaches, with the aim of refining surgical decision-making for this specific injury pattern.
METHODS
Clinical data
A total of 288 patients diagnosed with multiple rib fractures in the Department of Thoracic Surgery at Binhai County People’s Hospital between June 2018 and June 2024 were initially reviewed. Among them, 86 patients who underwent thoracoscopic internal fixation surgery were included in this study. Based on the surgical approach, patients were allocated into two groups: Complete Thoracoscopy group (n = 40), which underwent complete thoracoscopic internal fixation, and Thoracoscopy-Assisted group (n = 46), which underwent thoracoscopy-assisted surgery for fixation. The cohort comprised 61 males and 25 females, with an age range of 28 to 71 years and a mean age of 54.54 ± 9.06 years. Data on the cause of injury, fracture location, and number of fractured ribs were collected from medical records, imaging examinations, and three-dimensional rib reconstructions. Informed consent was obtained from all participants. This study was approved by the Medical Ethics Committee of Binhai County People’s Hospital (2025BYKYLL041) and the study design flowchart was shown in Figure 1.
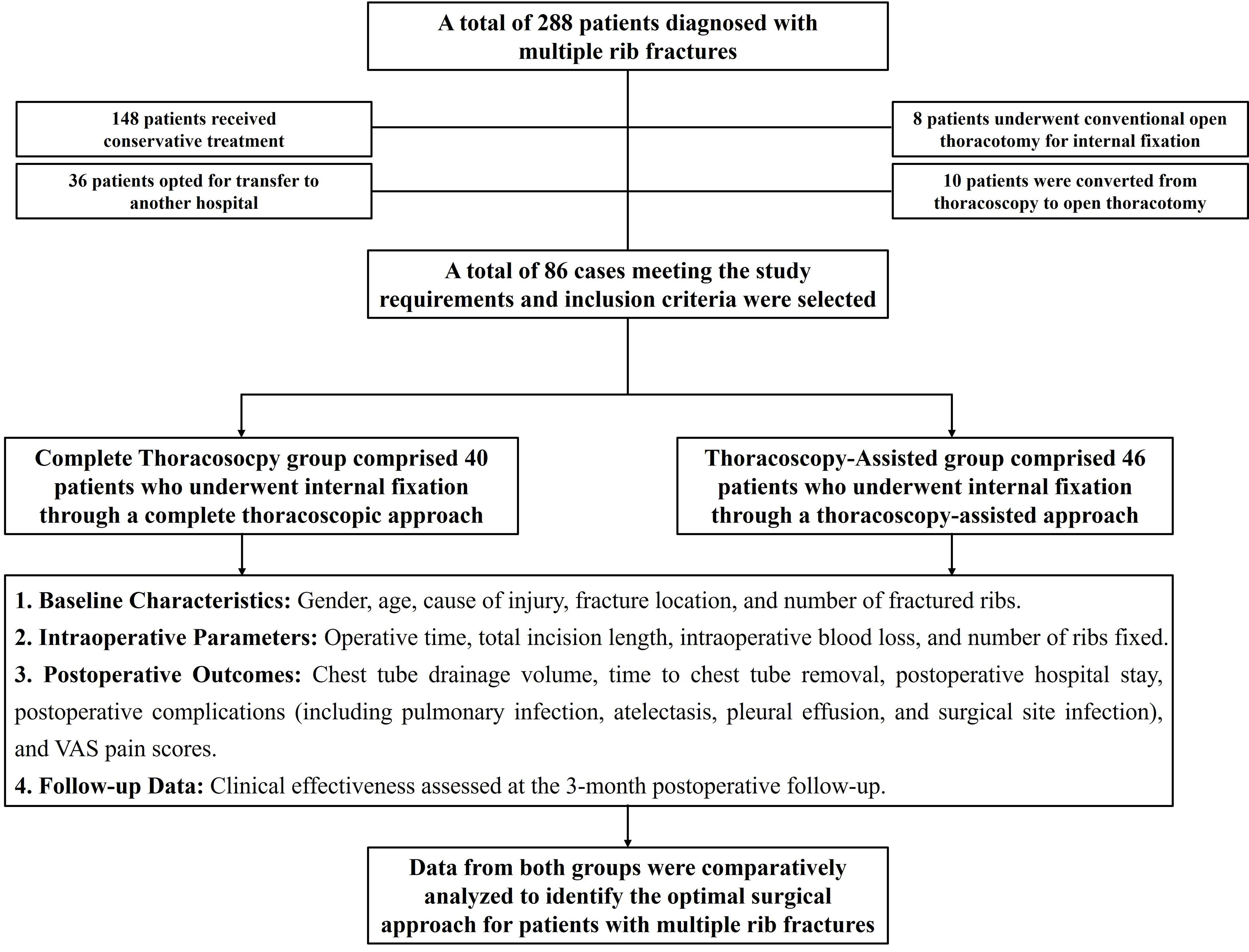
Figure 1. Overall design and implementation schematic diagram of the study. VAS: Visual Analog Scale.
Surgical grouping and study criteria
Indications for SSRF
According to the Chinese expert consensus[5], SSRF may be considered for non-flail chest rib fractures under the following conditions: (1) Fractures involving three or more ribs with significant displacement (Grade IIB recommendation); (2) Fractures requiring concurrent thoracic exploration for other surgical indications (Grade III recommendation); (3) Fractures accompanied by severe, intractable pain unresponsive to initial conservative management (Grade IIB recommendation).
Criteria for complete thoracoscopic surgery
The complete thoracoscopic approach was typically selected for patients meeting one or more of the following criteria[10]: (1) Young patients with significant chest wall deformity and high cosmetic concerns; (2) Patients prioritizing reduced hospital length of stay; (3) Fractures located in areas difficult to expose via open surgery, such as high posterior or paravertebral regions; (4) Patients with concomitant conditions requiring thoracic exploration; (5) Patients who actively and strongly requested a fully thoracoscopic procedure.
Inclusion and exclusion criteria
Inclusion criteria: (1) Diagnosis of rib fractures confirmed by chest computed tomography (CT) and three-dimensional reconstruction; (2) Presence of three or more fractured ribs with obvious displacement; (3) Hemodynamic stability, not requiring emergency surgery; (4) Availability of complete clinical data.
Exclusion Criteria: (1) Severe cardiac, hepatic, or renal dysfunction, or coagulation disorders; (2) Concurrent severe infection, particularly pulmonary infection; (3) Major associated injuries to the head, abdomen, spine, or limbs; (4) Patients undergoing bilateral SSRF; (5) Presence of flail chest with respiratory insufficiency, rendering the patient unfit for surgery.
Surgical procedures
All patients underwent surgery within two weeks of injury. Following general anesthesia induction, one-lung ventilation was established via double-lumen endotracheal intubation. Standard surgical preparation and draping were performed. To ensure comparability between groups, all operations were conducted by chief surgeons with equivalent seniority, qualifications, and technical expertise.
Complete Thoracoscopy group
The patient was placed in a lateral decubitus position with the affected side up. An approximately 4.0-cm incision was made on the affected side as the main operating port. The principle for selecting this incision was to maintain adequate spatial distance from the fracture sites to facilitate instrument manipulation. A 1.0-cm observation port was created in the 7th or 8th intercostal space at the mid-axillary line. Guided by preoperative localization [Figure 2A], the intercostal muscles, surrounding soft tissues, and periosteum adjacent to the fracture ends were dissected using an electrocautery hook under thoracoscopic visualization to adequately expose the rib fragments [Figure 2B]. After identifying the ribs requiring fixation, a dedicated “heart-shaped” reduction forceps was employed for anatomical reduction [Figure 2C]. A titanium-nickel (TiNi) shape memory alloy embracing fixator of appropriate size [Manufacturer: Lanzhou Ximai Memory Alloy Co., Ltd.; Model: 6Z(12-24)-(80-120)] was then introduced to the target rib using a specialized thoracoscopic rib plate applicator [Figure 2D]. Firm pressure was applied to insert the clasps of the fixator over the upper and lower edges of the fractured rib. Sterile warm saline (45-50 °C) was irrigated over the device to induce shape recovery, securing the fixation [Figure 2E]. Finally, the thoracic cavity was irrigated, hemostasis was achieved, and lung recruitment was performed. The incisions were closed, and a chest tube was placed through the observation port connected to a drainage system, concluding the procedure.
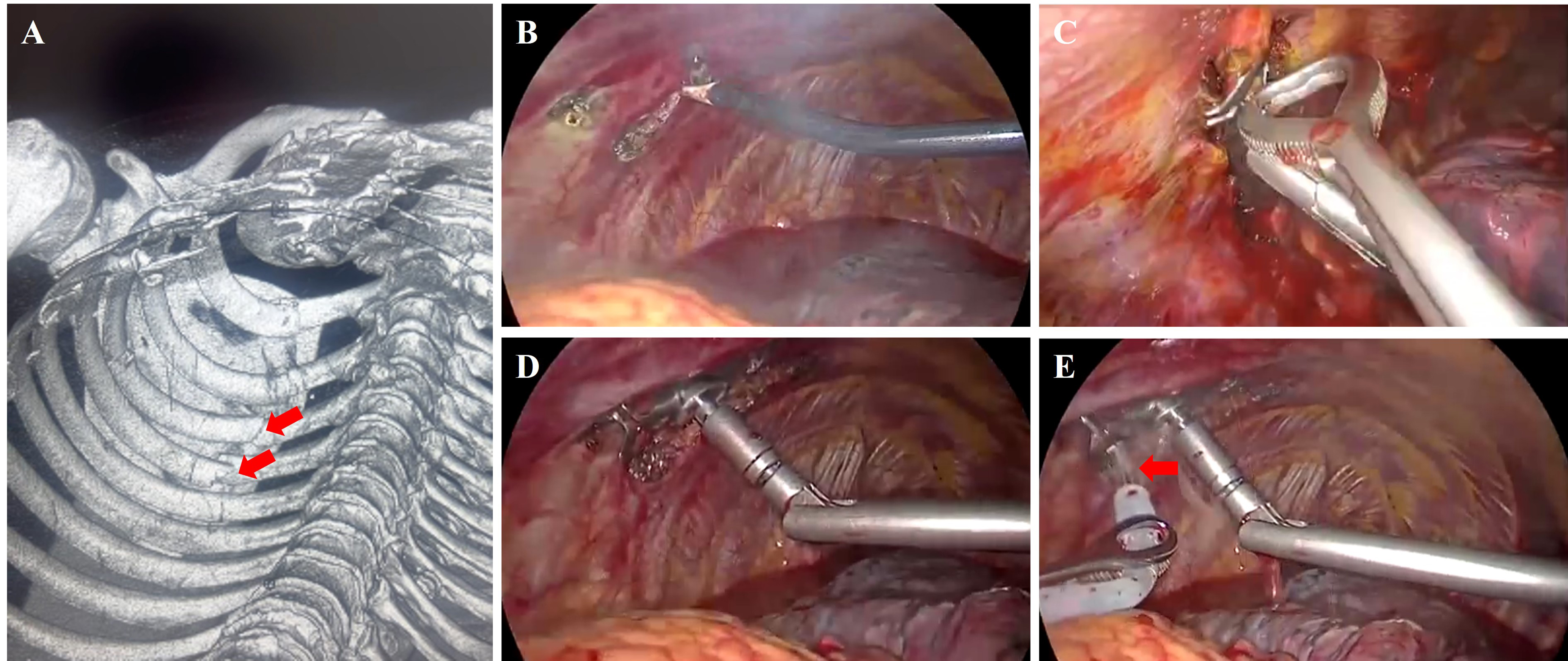
Figure 2. Intraoperative images of Complete Thoracoscopy group. (A) Preoperative three-dimensional reconstruction and fracture localization, the site of rib fracture and the fracture fragments were indicated by the red arrow; (B) Exposure of the fracture ends using an electrocautery hook; (C) “Heart-shaped” reduction forceps; (D) Specialized thoracoscopic rib plate applicator; (E) Application of sterile warm saline (indicated by the red arrow) to activate the shape memory alloy embracing fixator.
Thoracoscopy-Assisted group
The patient was positioned similarly. Based on preoperative imaging and 3D reconstruction models, the skin incision was planned and marked. An initial 4.0-5.0 cm incision was made along the rib axis, centered on the pre-marked point. Dissection proceeded along the upper border of the rib below, splitting the intercostal muscles to enter the pleural cavity. A thoracoscope was inserted to assess the rib fracture displacement [Figure 3A and B]. The incision was then extended, typically to 8.0-15.0 cm, guided by the preoperative CT findings and intraoperative exploration. The chest wall muscles were carefully mobilized, with detachment from rib attachments minimized to avoid muscle transection. The fracture ends were exposed, bone fragments were removed, and periosteal stripping was avoided. Following fracture reduction, fixation was achieved using a suitable TiNi shape memory alloy embracing fixator [Manufacturer: Lanzhou Ximai Memory Alloy Co., Ltd.; Model: 4HL II (10-16)-45H]. Under thoracoscopic guidance, the thoracic cavity was inspected, hemostasis was confirmed, and lung recruitment was performed. A chest tube was subsequently placed and connected to a drainage system, marking the end of the surgery [Figure 3C].
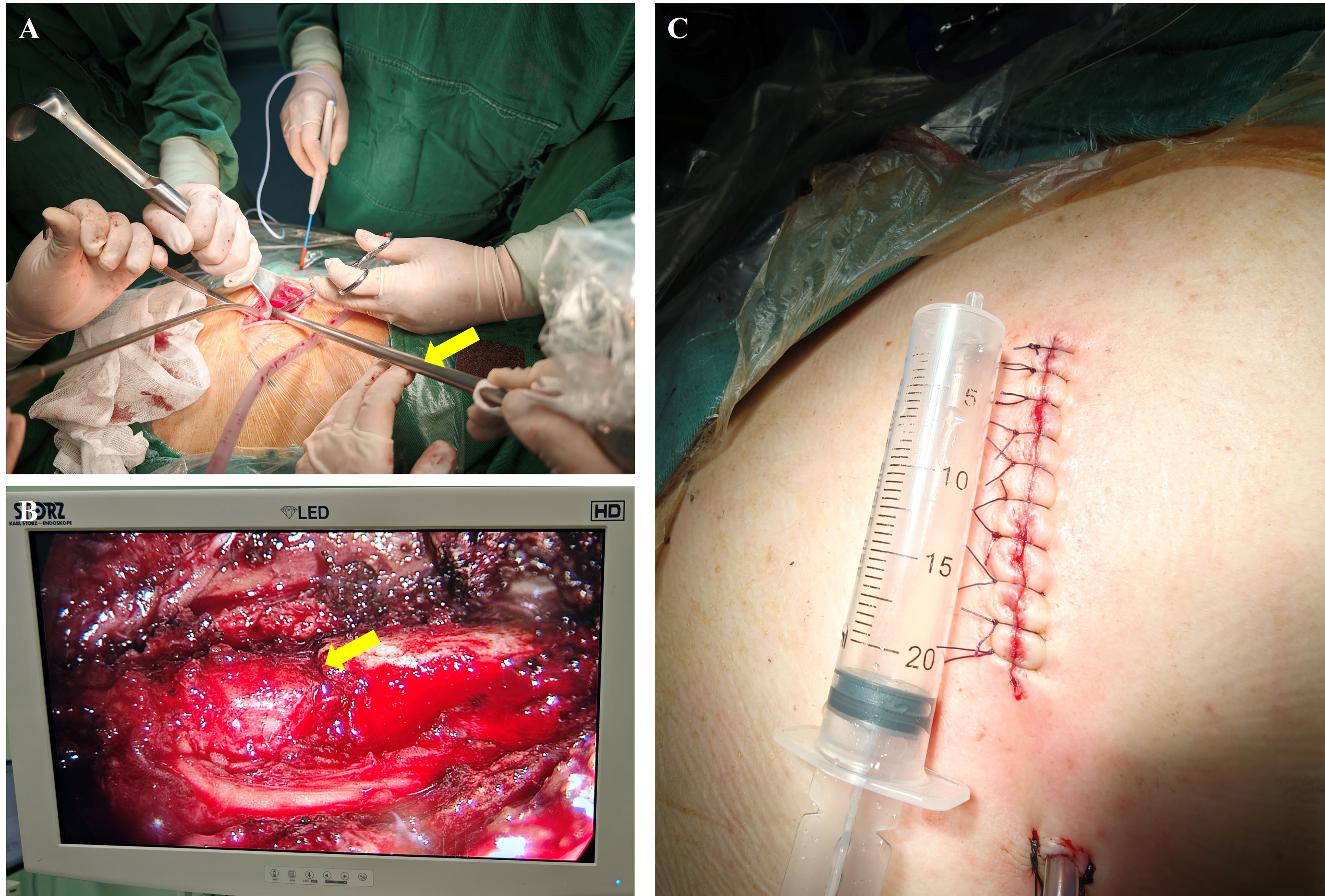
Figure 3. Intraoperative images of Thoracoscopy-Assisted surgery group. (A) Prior to extending the incision, a thoracoscope was inserted to evaluate the rib fractures, with the yellow arrow indicating the thoracoscope in situ; (B) Under thoracoscopy, the site of rib fracture and the fracture fragments were clearly visualized, as indicated by the yellow arrow; (C) The incision measures approximately 8 cm in length.
Clinical outcome measures
Surgical and perioperative parameters
The following surgical and perioperative parameters were recorded and compared between the two groups: operative time, total incision length, intraoperative blood loss, number of ribs fixed, postoperative chest tube drainage volume, time to chest tube removal, postoperative hospital stay, and complications (including pulmonary infection, atelectasis, pleural effusion, and surgical site infection).
Pain assessment
Pain severity was assessed using the Visual Analog Scale (VAS)[11]. Patients rated their pain on a scale from 0 to 10, where 0 indicated “no pain” and 10 represented “the worst pain imaginable”. VAS scores were collected preoperatively and on postoperative days 3 and 7.
Three-month postoperative clinical effectiveness
Clinical effectiveness was evaluated at three months postoperatively based on imaging findings and patient feedback. The outcomes were categorized as follows: Cured: No chest wall pain or paresthesia, and no respiratory dysfunction. Markedly Effective: Occasional mild chest wall pain or paresthesia, with no respiratory dysfunction. Improved: Intermittent mild chest wall pain or paresthesia, with mild respiratory dysfunction, and suboptimal chest wall cosmetic appearance. Ineffective: Persistent significant chest wall pain and paresthesia, respiratory dysfunction impacting daily life and work, and unsatisfactory chest wall appearance.
Statistical analysis
All statistical analyses were performed using SPSS software (version 22.0; IBM Corp.). Normality tests were conducted for the data in both groups, confirming that the data in both groups followed a normal distribution. Continuous data are presented as the mean ± standard deviation (x ± s). Comparisons between the two groups for continuous variables were conducted using Student’s t-test. Categorical data were analyzed using the Chi-square (χ²) test, with the Fisher-Freeman-Halton exact test applied when the assumptions for the χ² test were not met. A two-tailed P-value of less than 0.05 was considered statistically significant.
RESULTS
Comparison of baseline characteristics
There were no statistically significant differences between the two groups in terms of gender, age, cause of injury, post-traumatic complications, fracture sites, fracture location, or number of fractured ribs (P > 0.05). The detailed baseline data are presented in Table 1.
Comparison of baseline characteristics between the two groups
| Complete Thoracoscopy group (n = 40) | Thoracoscopy-Assisted group (n = 46) | χ2/t value | P-value | |
| Gender | 0.43 | 0.51 | ||
| Male | 27 | 34 | ||
| Female | 13 | 12 | ||
| Age | 53.12 ± 9.04 | 55.71 ± 10.68 | 1.18 | 0.24 |
| Cause of injury | 2.39 | 0.30 | ||
| Motor vehicle accident | 18 | 16 | ||
| Fall injury | 20 | 23 | ||
| Crush injury | 2 | 7 | ||
| Post-traumatic complications | 0.70 | 0.98 | ||
| Pneumothorax | 10 | 8 | ||
| Hemothorax | 4 | 6 | ||
| Hemopneumothorax | 4 | 6 | ||
| Subcutaneous emphysema | 8 | 9 | ||
| Pulmonary contusion | 10 | 12 | ||
| None | 4 | 5 | ||
| Fracture sites | 0.97 | 0.63 | ||
| Anterior | 21 | 23 | ||
| Lateral | 5 | 4 | ||
| Posterior | 14 | 19 | ||
| Fracture location | 0.32 | 0.56 | ||
| Unilateral | 37 | 44 | ||
| Bilateral (unilateral fixation) | 3 | 2 | ||
| Number of fractured ribs | 5.98 ± 2.03 | 6.34 ± 2.94 | 0.41 | 0.58 |
Comparison of surgical and perioperative outcomes
Compared with the Thoracoscopy-Assisted group, the Complete Thoracoscopy group demonstrated a significantly longer operative time but a shorter total incision length (P < 0.05). No statistically significant differences were observed between the two groups in terms of intraoperative blood loss, number of ribs fixed, postoperative chest tube drainage volume, time to chest tube removal, or postoperative hospital stay (P > 0.05). Furthermore, the incidence rates of postoperative complications, including pulmonary infection, pleural effusion, atelectasis, and surgical site infection, showed no significant differences between the groups (P > 0.05). Detailed data are presented in Table 2.
Comparison of surgical and perioperative outcomes between the two groups
| Complete Thoracoscopy group (n = 40) | Thoracoscopy-Assisted group (n = 46) | χ2/t value | P-value | |
| Operative time (min) | 120.80 ± 18.73 | 102.01 ± 24.02 | 2.33 | 0.03 |
| Intraoperative blood loss (mL) | 78.16 ± 18.71 | 86.03 ± 12.56 | 0.58 | 0.50 |
| Number of ribs fixed | 4.85 ± 1.13 | 4.40 ± 1.54 | 0.79 | 0.40 |
| Total incision length (cm) | 5.38 ± 1.34 | 10.58 ± 3.00 | 6.84 | < 0.01 |
| Postoperative chest tube drainage volume (mL) | 526.30 ± 108.04 | 552.51 ± 186.41 | 1.01 | 0.20 |
| Time to chest tube removal (day) | 5.62 ± 1.28 | 5.91 ± 2.28 | 0.80 | 0.34 |
| Postoperative hospital stay (day) | 7.64 ± 2.12 | 8.08 ± 2.36 | 1.24 | 0.20 |
| Postoperative complications | 5 | 9 | 0.65 | 0.41 |
| Pulmonary infection | 1 | 2 | ||
| Pleural effusion | 3 | 1 | ||
| Atelectasis | 1 | 3 | ||
| Surgical site infection | 0 | 3 |
Comparison of preoperative and postoperative VAS scores
No significant difference was found in preoperative VAS scores between the two groups (P = 0.3677). VAS scores on postoperative days 3 and 7 were significantly lower than preoperative scores in both groups (P < 0.05). Notably, the Complete Thoracoscopy group exhibited significantly lower VAS scores compared to the Thoracoscopy-Assisted group at both postoperative day 3 and day 7 (P < 0.05). The detailed data are presented in Table 3.
Comparison of VAS pain scores between the two groups at baseline and on post-operative days 3 and 7
| Preoperative | Post-operative D-3 | Post-operative D-7 | F | P-value (within-group) | |
| Complete Thoracoscopy group | 6.23 ± 0.61 | 4.08 ± 0.37*,# | 2.24 ± 0.56*,# | 14.54 | < 0.01 |
| Thoracoscopy-Assisted group | 6.28 ± 0.56 | 4.96 ± 0.51* | 2.87 ± 0.63* | 9.14 | < 0.01 |
| t | 0.91 | 3.72 | 3.02 | ||
| P-value (between-group) | 0.37 | < 0.01 | < 0.01 |
Comparison of postoperative effectiveness
All patients completed the 3-month postoperative follow-up. During this period, no complications such as implant displacement were observed in either group. Based on imaging assessment and patient-reported outcomes, the Complete Thoracoscopy group demonstrated significantly superior clinical effectiveness at the 3-month follow-up compared to the Thoracoscopy-Assisted group (P < 0.05). The detailed data are presented in Table 4.
Comparison of clinical effectiveness at the 3-month follow-up between the two groups
| Cured | Markedly effective | Improved | Ineffective | χ2 | P | |
| Complete Thoracoscopy group | 28 | 10 | 2 | 0 | 10.66 | < 0.01 |
| Thoracoscopy-Assisted group | 16 | 24 | 6 | 0 |
DISCUSSION
Rib fracture, as the most prevalent type of thoracic trauma, exhibits distinct global epidemiological patterns, with East Asia and high-income North America identified as key high-incidence regions. In terms of absolute case numbers, China currently bears the highest global disease burden. Projections indicate that the worldwide burden of rib fractures will continue to rise through 2030[12], accounting for approximately 10% of all chest trauma-related hospitalizations[13,14]. Historically, rib fractures have been classified by complexity into simple, multiple, and flail chest injuries, with severity varying substantially across categories. While most injuries can be managed successfully through either nonoperative or surgical treatment, optimal therapeutic strategies depend on fracture characteristics and associated clinical complications[15]. Conservative approaches, such as chest wall strapping, rib traction, and ventilator support, are often associated with several drawbacks including a high incidence of complications, prolonged treatment duration, significant pain, and delayed healing. In contrast, a growing body of evidence demonstrates that surgical stabilization for multiple rib fractures, particularly in flail chest, can significantly alleviate pain, improve ventilation, reduce dependence on mechanical ventilation and the incidence of pulmonary complications, and decrease hospital length of stay, mortality, and disability rates[16-18].
Traditional ORIF for rib fractures presents notable disadvantages, such as extensive incisions, substantial tissue trauma, prolonged postoperative recovery, and a high rate of complications[9]. With continuous advancements in thoracoscopic techniques, their application in the emergency management of thoracic trauma has become increasingly widespread. Compared to conventional open surgery, thoracoscopy offers two major advantages: (1) Although imaging modalities like CT three-dimensional reconstruction and ultrasound can localize fracture sites preoperatively, intraoperative displacement may still occur. Thoracoscopic visualization enables precise intraoperative localization of rib fractures, facilitating optimal incision planning and minimizing incision length; (2) It provides superior capability for exploring and managing associated intrathoracic injuries, including hemothorax, lung lacerations, diaphragmatic rupture, and intercostal artery injury[8]. Thoracoscopy enables genuine muscle‑sparing surgery by avoiding transection of major chest wall muscles or forceful retraction of the scapula, thereby largely preserving shoulder girdle function. Furthermore, the panoramic intrathoracic view allows not only fracture fixation but also comprehensive assessment of pulmonary contusion and management of active bleeding or organized hemothorax. More importantly, the reduced muscular trauma leads to significantly less postoperative pain, which encourages early and effective coughing and consequently markedly lowers the risk of pulmonary complications such as pneumonia[19]. Recently, Huang et al. conducted a comparative clinical study on this topic, further highlighting the clinical benefits of total thoracoscopic surgery[20].
A variety of rib-fixation systems, including claw-shaped plates, screw-and-plate constructs, and intramedullary devices, have been introduced worldwide, each with inherent advantages and limitations[21-23]. In the present study, the Complete Thoracoscopy group was treated with a TiNi shape-memory alloy claw that has gained increasing clinical acceptance[10,24]. The device obviates the need for drilling or cable-tying, thereby simplifying instrumentation. Manufactured from nickel-titanium alloy, it offers superior biocompatibility, corrosion resistance, and MRI compatibility, while eliciting minimal immune response. Its temperature-dependent memory property allows intra-operative deformation under cold saline and automatic restoration to its pre-set configuration at body temperature, generating continuous, dynamic compression across the fracture site. In contrast to conventional rigid plates, the TiNi-claw incorporates a reversed-arch design that increases its transverse diameter, creating a “neurovascular window” that protects the intercostal bundle. Consequently, fixation forces are redirected to the lateral cortical surface of the rib, reducing the risk of chronic post-operative chest-wall pain[10].
In a case-control study, Wang et al. demonstrated significant differences between thoracoscopic and conventional open surgical treatment for rib fractures[25]. The thoracoscopic approach was associated with a lower incidence of postoperative complications, along with favorable outcomes in terms of operative time, intraoperative blood loss, and incision length. Patients reported markedly reduced postoperative pain and significantly improved quality of life. While completely thoracoscopic rib fracture fixation was shown to be a safe, feasible, and minimally invasive method for mid-and posterior rib fractures covered by the scapula and thick dorsal muscles, the incidence of postoperative fracture malalignment was noted to be higher than anticipated[26]. In another retrospective analysis, Qian et al. evaluated outcomes of complete thoracoscopic surgery for multiple rib fractures or flail chest accompanied by severe thoracic trauma[27]. Their results indicated no statistically significant differences (P > 0.05) between groups in operative time, intraoperative blood loss, chest tube drainage volume, postoperative ventilator days, ICU length of stay, or total hospital stay. Although the overall postoperative complication rate did not differ significantly (P = 0.358), the incidence of pleural effusion was lower in the thoracoscopic group compared with the open surgery group (P = 0.025). Moreover, VAS pain scores on postoperative day 7 were significantly lower in the thoracoscopic group (P = 0.014). Thoracoscopically assisted rib fracture fixation represents a hybrid technique that combines conventional open surgical exposure with thoracoscopic visualization. While maintaining an external incision for fracture reduction and fixation, the procedure utilizes intra-thoracic endoscopic guidance, particularly advantageous in complex fractures and cases requiring simultaneous management of intrathoracic injuries. This approach enhances intraoperative visualization during fixation, facilitates hematoma evacuation, and may potentially reduce perioperative complications[28]. A prospective study reported that the thoracoscopically assisted group had shorter ventilator use (3.19 ± 3.37 days vs. 8.05 ± 8.23 days, P = 0.002) and a significantly lower incidence of pneumonia (38.1% vs. 75.0%, P = 0.005). Hospital stay was also notably shorter in the intervention group (17.76 ± 8.38 days vs. 24.13 ± 9.80 days, P = 0.011). These findings suggest that rib fixation combined with video-assisted thoracoscopic surgery (VATS) in severe blunt thoracic trauma with acute respiratory failure can shorten ventilator dependence, reduce pneumonia rates, and decrease overall hospitalization time[29].
In our retrospective analysis, we moved beyond the traditional open surgical approach for rib fractures and focused specifically on comparing complete thoracoscopy vs. thoracoscopy-assisted surgery in the treatment of multiple rib fractures in non-flail chest. Baseline demographic and clinical characteristics showed no significant differences between the two groups, confirming comparability. No statistically significant differences were observed in key perioperative indicators, including the number of fractured ribs fixed intraoperatively, postoperative chest-tube drainage volume, time to drain removal, and length of hospital stay. Furthermore, the incidence of common postoperative complications, such as pulmonary infection, pleural effusion, atelectasis, and surgical site infection, did not differ significantly between the two groups. It is noteworthy, however, that while the difference in the incidence of surgical site infection between the two groups did not reach statistical significance, not a single case of surgical site infection was observed in the Complete Thoracoscopy group. This observation, albeit derived from a limited sample, suggests a potential clinical trend favoring the complete thoracoscopic approach. The absence of surgical site infection in this cohort may partially reflect the inherent advantages of a minimally invasive technique, which typically involves smaller incisions, reduced tissue trauma, and potentially lower risk of wound complications, thereby contributing to enhanced postoperative recovery. This is also consistent with the finding in our study that the Complete Thoracoscopy group had significantly shorter skin incisions, implying reduced chest-wall trauma. Pre-operative VAS scores were identical; however, values on post-operative days 3 and 7 were lower in both groups relative to baseline, confirming that surgical stabilization abbreviates the painful period. Importantly, VAS scores at both time-points were significantly lower in the Complete Thoracoscopy group, an effect attributed to limited muscular and neural injury. Operative time was marginally longer in the Complete Thoracoscopy group, a predictable consequence of the learning curve associated with the adoption of a novel, fully endoscopic technique. We anticipate that accumulated experience will shorten operative times to, or even below, those required for the hybrid approach. At 3-month follow-up, no implant failure, respiratory dysfunction, or chest-wall deformity was encountered. Patients in the Complete Thoracoscopy group reported less frequent residual pain and hypo-aesthesia, reflecting the clinical benefits of minimized surgical trauma. Collectively, these data indicate that complete thoracoscopic SSRF with TiNi-claws reduces surgical insult, preserves shoulder-girdle function, and attenuates early and intermediate pain and dysesthesia compared with the thoracoscopy-assisted technique. Furthermore, with the deepening integration of medicine and engineering, a growing number of novel materials and technologies are being translated into preliminary clinical studies and applications for the internal fixation of rib fractures[30,31]. Concurrently, the continued maturation of artificial intelligence and 3D printing technologies holds significant promise for improving surgical outcomes for patients with rib fractures[32].
Several limitations of this study should be acknowledged. First, as a single-center investigation with a relatively small sample size, the statistical analyses may be subject to bias. Beyond that, the choice between complete thoracoscopy and thoracoscopy-assisted surgery was based on surgeon assessment, fracture pattern, and patient characteristics and preferences, rather than random allocation. This introduces a potential selection bias. Specifically, the complete thoracoscopy cohort included a higher proportion of younger patients, who may possess inherently better recovery potential and different pain perceptions. Although we ensured baseline comparability between the two groups, residual confounding from unmeasured factors (e.g., preoperative fitness, psychosocial factors) cannot be ruled out. Consequently, the observed advantages of complete thoracoscopy in VAS scores and patient satisfaction should be interpreted with caution, as they may be partially attributable to these baseline demographic and motivational differences rather than the surgical approach alone. Future prospective, randomized trials involving larger, multicenter cohorts are warranted to definitively isolate the effect of the surgical technique and validate our findings. Additionally, the follow-up period was limited, with clinical outcomes assessed only at three months postoperatively. Consequently, the long-term effectiveness of the two surgical approaches could not be evaluated. Future studies should incorporate extended follow-up durations to address this gap.
In conclusion, both complete thoracoscopic and thoracoscopy-assisted mini- incision approaches demonstrate satisfactory surgical outcomes for the treatment of multiple rib fractures. The complete thoracoscopic technique is associated with minimized surgical trauma, reduced postoperative pain, and improved clinical effectiveness in the short term, supporting its broader clinical application.
DECLARATIONS
Authors’ contributions
Made substantial contributions to the conception and design of the study: Wang S
Contributed to collecting data and writing the manuscript: Wang S, Zhang X, Shan Y
Performed revisions and provided administrative support: Zhang X, Shi Q
Served as supervising author: Shi Q
Availability of data and materials
All data are available from the corresponding author upon reasonable request.
AI and AI-assisted tools statement
Not applicable.
Financial support and sponsorship
This study was supported by the Yangzhou Science and Technology Project (YZ2023126) and the Yangzhou Foundation for Basic Research (Joint Program) (2024-2-07).
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and consent to participate
This study was approved by the Medical Ethics Committee of Binhai County People’s Hospital (Ethics approval number: 2025BYKYLL041). All patients volunteered to participate in the study and signed informed consent forms.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
REFERENCES
1. Hisamune R, Kobayashi M, Nakasato K, et al. A meta-analysis and trial sequential analysis of randomised controlled trials comparing nonoperative and operative management of chest trauma with multiple rib fractures. World J Emerg Surg. 2024;19:11.
2. Sawyer E, Wullschleger M, Muller N, Muller M. Surgical rib fixation of multiple rib fractures and flail chest: a systematic review and meta-analysis. J Surg Res. 2022;276:221-34.
3. Craxford S, Owyang D, Marson B, et al. Surgical management of rib fractures after blunt trauma: a systematic review and meta-analysis of randomised controlled trials. Ann R Coll Surg Engl. 2022;104:249-56.
4. Sermonesi G, Bertelli R, Pieracci FM, et al. Surgical stabilization of rib fractures (SSRF): the WSES and CWIS position paper. World J Emerg Surg. 2024;19:33.
5. Chest Injury Research Society. Chinese consensus on diagnosis and treatment of traumatic rib and sternal fractures. Chin J Thorac Cardiovasc Surg. 2023;39:513-30.
6. Ali-Osman F, Mangram A, Sucher J, et al. Geriatric (G60) trauma patients with severe rib fractures: is muscle sparing minimally invasive thoracotomy rib fixation safe and does it improve post-operative pulmonary function? Am J Surg. 2018;216:46-51.
7. Castater C, Hazen B, Davis C, et al. Video-assisted thoracoscopic internal rib fixation. Am Surg. 2022;88:994-6.
8. Zhang J, Hong Q, Ma C. Complete VATS in rib fractures: more than just a minimally invasive procedure. Ann Thorac Surg. 2022;114:601-2.
9. Lin ZW, Long JT, Lin WK. Short-term follow-up of single-port thoracoscopic rib fracture reduction and internal fixation for the treatment of multiple rib fractures. Arch Orthop Trauma Surg. 2024;145:71.
10. Zhang J, Hong Q, Mo X, Ma C. Complete video-assisted thoracoscopic surgery for rib fractures: series of 35 cases. Ann Thorac Surg. 2022;113:452-8.
11. Boonstra AM, Schiphorst Preuper HR, Balk GA, Stewart RE. Cut-off points for mild, moderate, and severe pain on the visual analogue scale for pain in patients with chronic musculoskeletal pain. Pain. 2014;155:2545-50.
12. Wang Z, Cai Y, Tong Y, et al. Global, regional, and national burden of fracture of sternum and/or fracture of one or more ribs: a systematic analysis of incidence, YLDs with projections to 2030. Front Public Health. 2025;13:1565478.
13. Zhang Q, Song L, Ning S, Xie H, Li N, Wang Y. Recent advances in rib fracture fixation. J Thorac Dis. 2019;11:S1070-7.
14. Michelitsch C, Acklin YP, Hässig G, Sommer C, Furrer M. Operative stabilization of chest wall trauma: single-center report of initial management and long-term outcome. World J Surg. 2018;42:3918-26.
15. Franssen AJPM, Daemen JHT, Luyten JA, et al. Treatment of traumatic rib fractures: an overview of current evidence and future perspectives. J Thorac Dis. 2024;16:5399-408.
16. Kelley KM, Burgess J, Weireter L, et al. Early use of a chest trauma protocol in elderly patients with rib fractures improves pulmonary outcomes. Am Surg. 2019;85:288-91.
17. Li S, Wang C, Hu P, et al. Surgical management of multiple rib fractures in polytrauma patients: semi-damage control surgery. Int J Med Sci. 2024;21:2926-33.
18. Doben AR, Schubl SD, Dudaryk R. Surgical rib fixation in traumatic rib fractures: is it warranted? Curr Opin Anaesthesiol. 2022;35:172-5.
19. Daemen JHT, Verkoulen KCHA, Geenen L, et al. Reconsidering rib fixation: is a complete video-assisted thoracoscopic surgery approach the future for surgical stabilization? J Thorac Dis. 2025;17:6348-50.
20. Huang X, Wang D, Jiang X, et al. Comparative clinical study of total thoracoscopic surgery and thoracoscopy-assisted small-incision surgery for multiple rib fractures. Sci Rep. 2026;16:14559.
21. Bottlang M, Walleser S, Noll M, et al. Biomechanical rationale and evaluation of an implant system for rib fracture fixation. Eur J Trauma Emerg Surg. 2010;36:417-26.
22. Pieracci FM, Johnson JL, Stovall RT, Jurkovich GJ. Completely thoracoscopic, intra-pleural reduction and fixation of severe rib fractures. Trauma Case Rep. 2015;1:39-43.
23. la Rosa AL, Mosiñoz-Montes R, Matehuala-García J, Román-Guzmán E, Quero-Sandoval F, Reyes-Miranda AL. [Unstable thorax fixation with bioabsorbable plates and screws. Presentation of some cases]. Cir Cir. 2015;83:23-8.
24. Wang J, Sun Z, Liu Y, et al. Clinical effect of the internal fixation for rib fracture with single utility port complete video-assisted thoracoscopic surgery. J Cardiothorac Surg. 2024;19:59.
25. Wang D, Xu Y, Wang Q, Xu Y, Wang X. A cohort study on the comparison of complications, short-term efficacy, and quality of life between thoracoscopic surgery and traditional surgery in the treatment of rib fractures. Contrast Media Mol Imaging. 2022;2022:2079098.
26. Yang Y, Xie Z, Zhang J, et al. Completely thoracoscopic surgical stabilization of rib fractures: balancing minimally invasive benefits against technique-specific complications: a single-center retrospective study. World J Emerg Surg. 2025;20:54.
27. Qian G, Mao Y, He J, Gao L. Outcomes of internal rib fixation through complete video-assisted thoracoscopic surgery for multiple rib fractures and flail chest in severe chest trauma. Eur J Trauma Emerg Surg. 2025;51:2.
28. Kayata H, Usui A, Terakawa K, et al. Feasibility and efficacy of video-assisted thoracoscopic surgery for the surgical stabilization of rib fractures: a single-center retrospective cohort study. Eur J Trauma Emerg Surg. 2025;51:277.
29. Wu TH, Lin HL, Chou YP, Huang FD, Huang WY, Tarng YW. Facilitating ventilator weaning through rib fixation combined with video-assisted thoracoscopic surgery in severe blunt chest injury with acute respiratory failure. Crit Care. 2020;24:49.
30. Bauman ZM, Tian Y, Puthoff G, Whitbeck SA, Gardner S, White TW. An early analysis of polyetheretherketone (PEEK) plates for the surgical stabilization of rib fractures: a pilot study. Injury. 2024;55:111969.
31. Fukunaga N, Sato H, Wakami T, et al. Fixation devices made of poly-L-lactide composite for rib reconstruction after thoracotomy. J Cardiothorac Surg. 2024;19:130.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Copyright

Data & Comments
Data
0












Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].