


The impact of phthalate exposure on cardiometabolic risk progression in children and the modifying role of movement behaviors
 0
0 Abstract
Background: Phthalate exposure has been linked to adverse cardiometabolic profiles in children, but its association with longitudinal cardiometabolic risk patterns and the modifying role of 24-h movement behaviors remain unclear.
Methods: We analyzed repeated follow-up data from a school-based cohort of Chinese children from 2018 to 2020. Urinary phthalate metabolites were measured annually and averaged to represent habitual exposure. Cardiometabolic risk status was classified into five progression patterns: stable healthy, improving, fluctuating, worsening, and persistently abnormal. Multinomial logistic regression was used to examine associations between phthalate exposure quartiles and progression patterns. Effect modification by sex and adherence to the 24-h movement guidelines was evaluated, and weighted quantile sum regression was used to assess mixture effects.
Results: Most phthalate metabolites showed limited or inconsistent associations with stable healthy, improving, or fluctuating patterns. In contrast, higher exposure to several high-molecular-weight phthalate metabolites was associated with increased odds of the persistently abnormal pattern, particularly for MEOHP and MEHHP. Associations with worsening patterns were generally inconsistent. Sex-stratified analyses suggested stronger associations among boys, although formal interaction evidence was limited. Adherence to the 24-h movement guidelines was associated with weaker exposure-outcome associations, but estimates were imprecise. Mixture analyses showed a positive association between overall phthalate exposure burden and the persistently abnormal pattern.
Conclusions: Repeated phthalate exposure was mainly associated with persistently abnormal cardiometabolic risk in children. Healthy movement behaviors may partly mitigate these associations, although further longitudinal studies are needed.
Keywords
INTRODUCTION
The growing prevalence of cardiometabolic risk factors among children and adolescents has become a major global public health concern. Cardiometabolic abnormalities rarely occur in isolation; rather, they tend to cluster as a constellation of interrelated risk factors, including dyslipidemia, elevated blood pressure, impaired glucose metabolism, and central obesity. Previous studies have shown that cardiometabolic abnormalities identified in childhood often persist over time and may track into adulthood, thereby increasing the risk of cardiovascular target organ damage and related diseases later in life[1-3]. However, cardiometabolic health in children is not static. During growth and development, cardiometabolic status may follow heterogeneous trajectories, and studies relying on single-time-point assessments are insufficient to capture these dynamic changes. A life-course perspective that considers the evolution of cardiometabolic risk patterns is therefore increasingly recognized as essential for early prevention research.
Although earlier research has primarily focused on individual outcomes such as obesity, dyslipidemia, or metabolic syndrome, accumulating evidence suggests that cardiometabolic health during childhood is characterized by substantial variability and developmental heterogeneity[4,5]. Some children maintain a metabolically healthy profile over time, whereas others may improve, deteriorate, or remain persistently abnormal. In recent years, trajectory- and pattern-based approaches have been increasingly applied in pediatric populations to characterize longitudinal changes in metabolic risk and related behaviors[4,6,7]. These approaches provide more informative insights into long-term cardiometabolic outcomes than traditional cross-sectional assessments. Nevertheless, most existing studies have focused primarily on anthropometric or metabolic indicators themselves, with limited attention to environmental determinants that may shape these longitudinal risk patterns. Understanding cardiometabolic risk from a progression-pattern perspective while incorporating environmental exposures is therefore critical for elucidating early disease development and informing targeted prevention strategies[1].
Among environmental determinants, phthalates are widely used plasticizers commonly found in food packaging materials, personal care products, and medical devices, resulting in ubiquitous human exposure. Children are considered particularly vulnerable due to their higher exposure frequency and immature metabolic regulation systems[8,9]. Evidence from the U.S. National Health and Nutrition Examination Survey (NHANES) has demonstrated associations between certain phthalate metabolites and adiposity or metabolic syndrome-related profiles in adolescents and adults[10]. Findings from European longitudinal and birth cohort studies further suggest that early-life or sustained phthalate exposure may be associated with childhood adiposity and cardiometabolic traits, with potential sex-specific differences[11,12]. Mechanistic studies indicate that phthalates may disrupt endocrine signaling, lipid metabolism, inflammatory responses, and epigenetic regulation, all of which are key pathways underlying cardiometabolic dysfunction. In addition, recent mixture-based and epigenetic studies suggest that phthalates may influence metabolic regulatory networks and contribute to cardiometabolic risk development[13-15]. Despite this growing body of evidence, most epidemiological studies have relied on cross-sectional designs or single-outcome analyses, and the associations between phthalate exposure and longitudinal cardiometabolic risk progression patterns in children remain insufficiently explored[8].
Beyond environmental exposures, lifestyle behaviors play a crucial role in pediatric cardiometabolic health. The 24-h movement guidelines emphasize the integrated assessment of physical activity, sedentary behavior, and sleep across the entire day and have been incorporated into public health recommendations[16]. Previous studies have shown that adherence to these guidelines is associated with more favorable cardiometabolic profiles in children and adolescents, although overall adherence remains suboptimal[17,18]. Emerging evidence also suggests that lifestyle behaviors may modify individual susceptibility to environmental exposures, potentially influencing the strength of associations between environmental chemicals and metabolic outcomes[19]. Nevertheless, evidence regarding whether 24-h movement patterns can modify the relationship between phthalate exposure and long-term cardiometabolic risk progression in children is still limited.
Against this background, the present study draws on longitudinal data from a well-established pediatric cohort in Xiamen, China. Using a progression-pattern framework, we first characterize distinct trajectories of cardiometabolic risk development during childhood. We then examine the associations between phthalate exposure and these cardiometabolic risk progression patterns. In addition, we evaluated potential effect modification by sex and adherence to the 24-h movement guidelines. By integrating environmental exposures, behavioral factors, and longitudinal cardiometabolic patterns, this study aims to provide novel evidence on the long-term evolution of cardiometabolic risk in childhood and to inform comprehensive strategies for early prevention.
METHODS
Study population
This study was a school-based longitudinal cohort conducted in Xiamen, Fujian Province, China. A multistage cluster sampling design was used to recruit school-aged children from four nine-year compulsory education schools. The initial recruitment phase was carried out in October 2017, during which approximately 2,298 students in grades 2 to 4 participated in baseline screening, including physical examinations and questionnaire surveys. According to the study protocol, children with severe systemic diseases (e.g., cardiovascular, hepatic, or renal diseases), diagnosed endocrine disorders, those who had already entered puberty, or those unwilling to participate in long-term follow-up and biospecimen collection were excluded. In May 2018, the longitudinal cohort was formally established, and a total of 772 children who met the inclusion criteria were enrolled. The participant selection process is illustrated in Supplementary Figure 1. The year 2018 was defined as the baseline for the present analysis. Participants were followed annually from 2018 to 2020, with each follow-up visit including standardized physical examinations, questionnaire surveys, and biological sample collection. All data were collected according to uniform standardized procedures with strict quality control.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Peking University (approval number: IRB00001052-17026). Written informed consent was obtained from all participants and their legal guardians prior to enrollment.
Measurement of urinary phthalate metabolites
Urine samples were collected by trained research staff at schools using polypropylene containers free of phthalates. Samples were immediately stored under low-temperature conditions and transported to the laboratory, where they were stored at -80°C until analysis. Phthalate metabolites were measured at the Peking University Medical Laboratory using an ultra-performance liquid chromatography-tandem triple quadrupole mass spectrometry (UPLC-MS/MS) method. This method has been validated and widely applied in population-based studies and is known for its high sensitivity and reproducibility[20-22].
Seven commonly detected phthalate metabolites were measured, including monomethyl phthalate (MMP), monoethyl phthalate (MEP), mono-n-butyl phthalate (MBP), monoisobutyl phthalate (MiBP), mono-2-ethylhexyl phthalate (MEHP), mono-2-ethyl-5-hydroxyhexyl phthalate (MEHHP), and mono-2-ethyl-5-oxohexyl phthalate (MEOHP). Sample pretreatment and quality control procedures, including enzymatic deconjugation, purification, and the use of blank and quality control samples, were conducted according to previously validated protocols. The limits of detection (LOD) and intra- and inter-batch coefficients of variation for all metabolites met established analytical quality control standards[23,24]. Concentrations below the LOD were imputed as LOD divided by the square root of two. Detailed information on LOD values and detection frequencies is provided in Supplementary Table 1.
To account for inter-individual variability in urinary dilution, a covariate-adjusted standardization approach proposed by O’Brien et al. was applied at the data processing and statistical analysis[25]. In this approach, urinary metabolite concentrations were adjusted using regression-based correction incorporating urinary creatinine and key demographic covariates (e.g., age, sex, and body mass index), rather than simple creatinine normalization, to reduce potential bias when creatinine is associated with metabolic outcomes[26]. In addition, a sensitivity analysis was conducted using conventional creatinine correction (ng/mmol creatinine) based on three-year averaged concentrations, with identical modeling procedures. Based on molecular weight and alkyl chain structure, phthalate metabolites were further classified into low-molecular-weight phthalates (LMWP; MMP, MEP, MBP, and MiBP) and high-molecular-weight phthalates (HMWP; primarily DEHP metabolites, including MEHP, MEHHP, and MEOHP). Molar concentrations within each group were summed to represent overall exposure and used in subsequent analyses. This grouping approach has been widely used in environmental epidemiology to evaluate exposure mixtures while acknowledging heterogeneity in biological effects across individual metabolites. Because urinary phthalate metabolites have relatively short biological half-lives and exhibit substantial within-person variability, concentrations measured at each annual visit (2018-2020) were first processed separately and then averaged across the three survey waves to characterize habitual exposure levels. This approach has been widely adopted in environmental epidemiological studies to reduce random measurement error associated with single-spot urine samples.
Outcome definition
At each follow-up visit, participants underwent standardized physical examinations and fasting venous blood collection to assess cardiometabolic risk factors. All physical examinations were conducted at schools by trained research staff following uniform protocols. Height and weight were measured using portable stadiometers and calibrated electronic scales, respectively. Waist circumference was measured at the end of normal expiration at a standardized anatomical site using a non-elastic tape. Blood pressure was measured with a standard mercury sphygmomanometer. All anthropometric and blood pressure measurements were performed twice, and the average values were used for analysis.
Fasting venous blood samples were collected between 7:00 and 9:00 a.m. after at least 10 h of overnight fasting. Samples were promptly centrifuged to separate serum and stored at -80 °C until analysis. Fasting blood glucose (FBG), triglycerides (TG), and high-density lipoprotein cholesterol (HDL-C) were measured using an automated biochemical analyzer, with all assays conducted in accordance with standardized laboratory quality control procedures.
Cardiometabolic risk factors were defined based on established literature and the latest Chinese pediatric diagnostic guidelines for cardiovascular health[27-30]. Central obesity was defined as waist circumference at or above the age- and sex-specific 90th percentile. Elevated blood pressure was defined as systolic and/or diastolic blood pressure at or above the age- and sex-specific 95th percentile. Hypertriglyceridemia was defined as TG ≥ 1.47 mmol/L, low HDL-C as HDL-C < 1.03 mmol/L, and elevated fasting glucose as FBG ≥ 5.6 mmol/L. The presence of any one of these five abnormalities at a given follow-up visit was considered indicative of abnormal cardiometabolic risk status. This definition was intended to capture early-stage metabolic dysregulation in children, where even a single abnormality may signal increased future cardiometabolic vulnerability.
Based on repeated assessments across follow-up visits, participants were further classified into five cardiometabolic risk progression patterns: (1) Participants who exhibited no abnormalities at all visits were classified as the stable healthy pattern. (2) Those with abnormalities at baseline or early follow-up who subsequently reverted to and maintained a normal status were classified as the improving pattern. (3) Participants without abnormalities at baseline who developed abnormalities during follow-up that persisted thereafter were classified as the worsening pattern. (4) Participants whose cardiometabolic status alternated between healthy and abnormal states across visits, without a sustained improving or worsening trend, were classified as the fluctuating pattern. (5) Participants who presented with at least one abnormality at baseline and at all subsequent visits were classified as the persistently abnormal pattern. This classification framework integrates information across multiple time points and captures the dynamic evolution of cardiometabolic risk during childhood. Compared with single-time-point assessments, such pattern-based approaches provide more informative insights into early cardiometabolic risk accumulation and its potential long-term implications.
Covariates and lifestyle factors
All covariates were collected using standardized questionnaires administered at baseline and during follow-up visits, completed jointly by children and their parents or legal guardians. Potential confounding variables included child sex (boy/girl), age (years), place of residence (urban/rural), only-child status (yes/no), mode of delivery (vaginal delivery/cesarean section), highest parental educational attainment (junior high school or below/high school or technical secondary school/college or above), and family history of cardiometabolic diseases (yes/no). These variables were selected based on prior literature suggesting their potential associations with cardiometabolic risk and environmental exposure patterns. In addition, pubertal development at baseline was assessed during routine school health examinations by trained clinicians using Tanner staging, based on the evaluation of secondary sexual characteristics and pubic hair development.
Lifestyle factors included physical activity, sedentary behavior, and sleep duration. Relevant information was collected using structured questionnaires at each follow-up visit. Physical activity was assessed as the average daily time spent in moderate-to-vigorous physical activity (MVPA). Sedentary behavior was evaluated based on daily recreational screen time, and sleep duration was calculated as the average nightly sleep time. To account for potential dietary confounding, several diet-related variables were also collected, including sugar-sweetened beverage intake, snack consumption, fried food consumption, and meat intake. Participants reported their average intake over the past seven days. Each variable was categorized into three levels (0 = low intake, 1 = moderate intake, and 2 = high intake) according to predefined intake ranges and included as ordinal covariates in sensitivity analyses.
Based on these three behavioral components, a composite indicator reflecting adherence to the 24-h movement guidelines was constructed. Participants were considered adherent if they simultaneously met all three recommendations: at least 60 min of MVPA per day, no more than 2 h of recreational screen time per day, and age-specific recommended sleep duration (9-11 h per night for school-aged children and 8-10 h per night for adolescents)[16,31]. This composite indicator was used to characterize overall lifestyle patterns and to evaluate potential effect modification in the association between phthalate exposure and cardiometabolic risk progression patterns.
Statistical analysis
Continuous variables were summarized as mean ± standard deviation or median (interquartile range), depending on distributional characteristics, and categorical variables were presented as counts and percentages. Differences in baseline characteristics between boys and girls were assessed using the t-test or Wilcoxon rank-sum test for continuous variables and the χ2 test for categorical variables.
Urinary phthalate metabolite concentrations were right-skewed and therefore natural log-transformed prior to analysis. To better reflect long-term exposure and reduce short-term variability inherent to spot urine samples, metabolite concentrations measured across the three follow-up waves (2018-2020) were averaged to construct three-year mean exposure indices. These averaged concentrations were further categorized into quartiles (Q1-Q4), with the lowest quartile serving as the reference group.
Multinomial logistic regression models were used to examine associations between phthalate exposure and cardiometabolic risk progression patterns, with the stable healthy pattern as the reference outcome. Odds ratios (ORs) and 95% confidence intervals (CIs) were estimated for the improving, fluctuating, worsening, and persistently abnormal patterns. Three models with increasing levels of adjustment were constructed: Model 1 was unadjusted; Model 2 adjusted for child sex, age, and residence; and Model 3 further adjusted for family history of cardiometabolic diseases, only-child status, mode of delivery, and parental educational attainment. Baseline cardiometabolic status was not included as a covariate because it is inherently incorporated into the definition of progression patterns, and adjusting for it would result in over-adjustment.
To evaluate potential sex-specific differences, both sex-stratified analyses and formal interaction tests (exposure × sex) were conducted based on Model 3. In addition, interaction terms were included to assess potential effect modification by adherence to the 24-h movement guidelines. The statistical significance of interaction terms was evaluated using Wald tests based on the multinomial logistic regression models. Weighted quantile sum (WQS) regression was further applied to assess the overall association between mixed phthalate exposure and cardiometabolic risk progression patterns. Phthalate metabolites were categorized into quartiles before inclusion in the WQS model. The dataset was randomly divided into training (40%) and validation (60%) subsets, and 1,000 bootstrap samples were used to estimate stable mixture weights. A positive-direction constraint was specified based on prior evidence suggesting predominantly adverse metabolic effects of phthalate exposure. The WQS index was incorporated into a multinomial logistic regression framework and adjusted for the same covariates as in the single-exposure models[18]. Given the relatively modest sample size, WQS results should be interpreted as exploratory.
All statistical analyses were conducted using R (version 4.3.2). All tests were two-sided, and P values < 0.05 were considered statistically significant.
RESULTS
Basic characteristics of participants
Table 1 summarizes the demographic and family characteristics of the study participants, which were generally comparable between boys and girls. The median age was slightly higher in boys than in girls (9.4 vs. 8.4 years, P < 0.001). No significant sex differences were observed for place of residence, only-child status, mode of delivery, parental educational attainment, or family history of cardiometabolic diseases (all P > 0.05). The distribution of cardiometabolic risk progression patterns during follow-up is presented in Figure 1. The stable healthy pattern was the most prevalent in both sexes. Although some differences in the distribution of progression patterns between boys and girls were observed descriptively, these differences were not formally tested and should be interpreted with caution. The baseline prevalence of individual cardiometabolic risk components is shown in Supplementary Table 2. Elevated fasting glucose was relatively uncommon in this cohort (1.2%), whereas central obesity was the most prevalent component (11.2%).
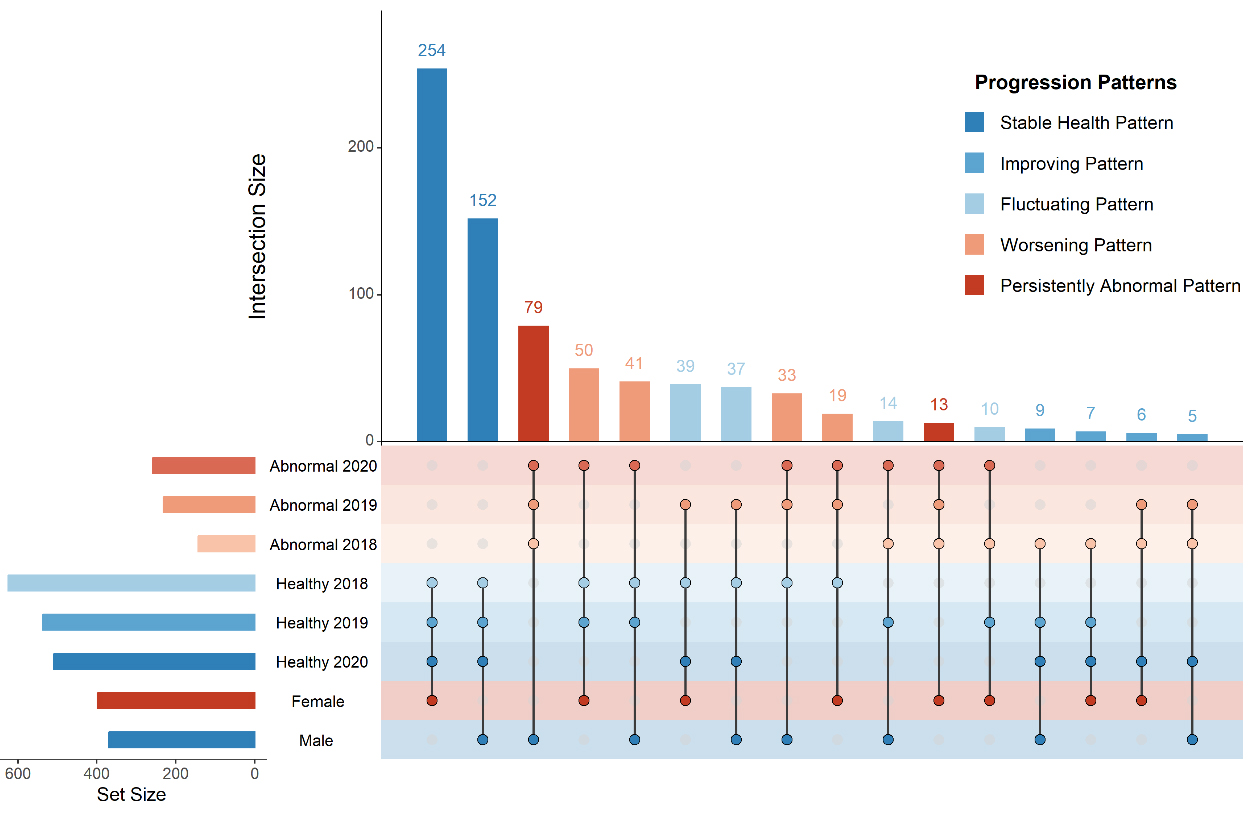
Figure 1. Cardiometabolic risk status progression patterns across the 2018-2020 follow-up period. Cardiometabolic risk progression patterns were defined based on repeated assessments across three follow-up visits. Each participant was classified into one of five patterns: stable healthy, improving, fluctuating, worsening, or persistently abnormal.
Basic characteristics of included participants, stratified by sex
| Characteristics | BoyN = 3731 | GirlN = 3991 | P-value2 |
| Age (years) | 9.4 (9.1, 10.0) | 8.4 (8.0, 8.9) | < 0.001 |
| Place of residence | 0.573 | ||
| Urban | 357.0 (95.7%) | 386.0 (96.7%) | |
| Rural | 16.0 (4.3%) | 13.0 (3.3%) | |
| Only-child status | 111.0 (29.8%) | 118.0 (29.6%) | > 0.999 |
| Mode of delivery | 0.765 | ||
| Vaginal delivery | 211.0 (56.6%) | 231.0 (57.9%) | |
| Cesarean section | 162.0 (43.4%) | 168.0 (42.1%) | |
| Mother’s educational attainment | 0.100 | ||
| Junior high school or below | 65.0 (17.4%) | 49.0 (12.3%) | |
| High school or technical secondary school | 88.0 (23.6%) | 91.0 (22.8%) | |
| College or above | 220.0 (59.0%) | 259.0 (64.9%) | |
| Father's educational attainment | 0.278 | ||
| Junior high school or below | 53.0 (14.2%) | 48.0 (12.0%) | |
| High school or technical secondary school | 90.0 (24.1%) | 83.0 (20.8%) | |
| College or above | 230.0 (61.7%) | 268.0 (67.2%) | |
| Family history of cardiometabolic diseases | 245.0 (65.7%) | 271.0 (67.9%) | 0.560 |
Associations between individual phthalate exposures and cardiometabolic risk progression patterns
The associations between individual phthalate exposures and cardiometabolic risk progression patterns are presented in Figure 2, with detailed estimates from different adjustment models provided in Supplementary Tables 3 and 4. Results from Models 1 and 2 are shown in Supplementary Figure 2, whereas Figure 2 presents the fully adjusted results from Model 3. Overall, the most consistent associations were observed for the persistently abnormal pattern, while associations with the improving and fluctuating patterns were generally weaker and less consistent across metabolites. In Model 3, most phthalate metabolites showed weak or inconsistent associations with the improving and fluctuating patterns, with odds ratios close to 1 and confidence intervals including the null value. These findings suggest limited evidence of stable associations for these patterns.
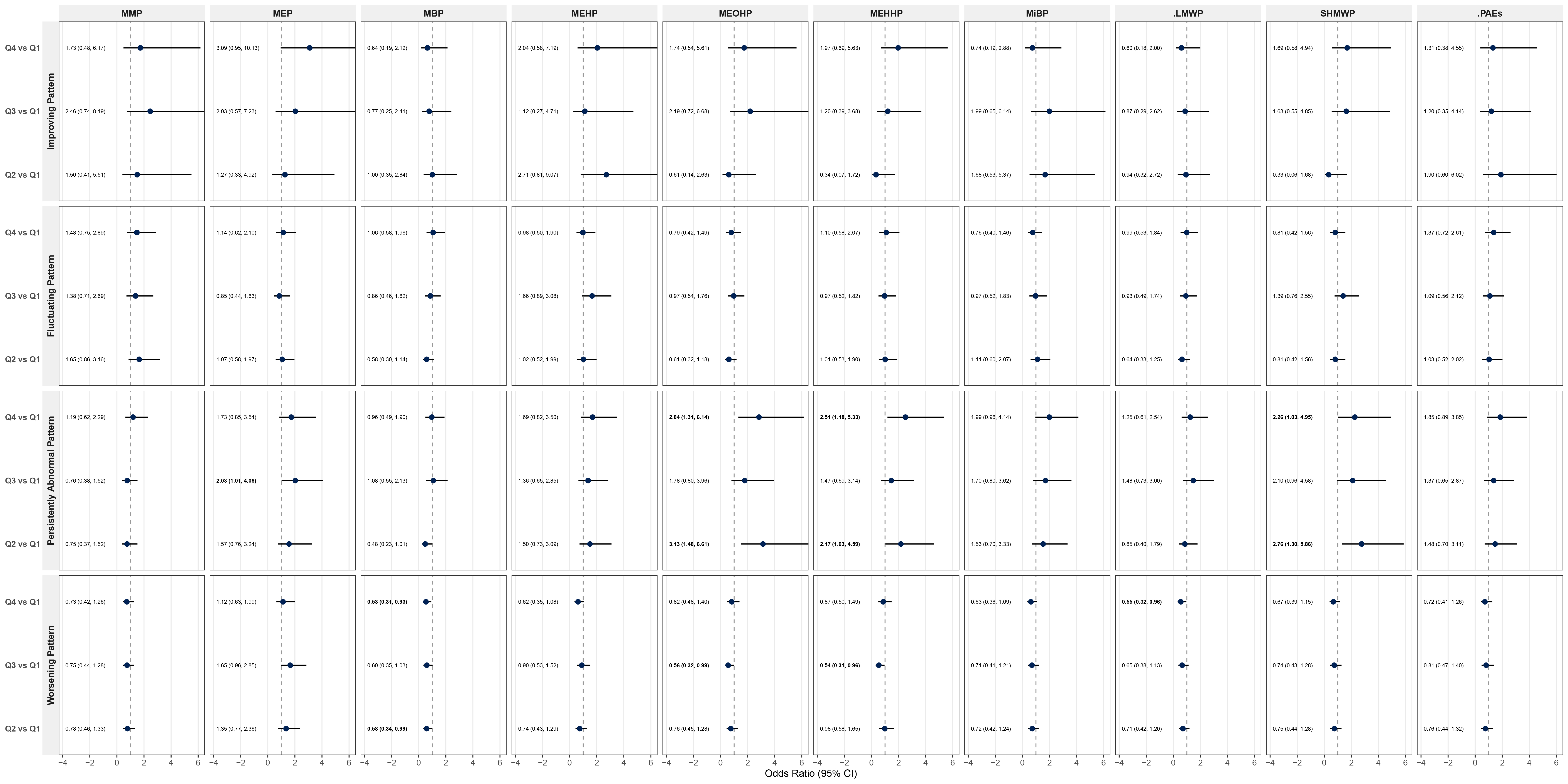
Figure 2. Association Between Phthalate Exposure and Cardiometabolic Risk Progression Patterns. (Multivariate Logistic Regression). Results from multinomial logistic regression models. Model 3 was adjusted for age, sex, residence, parental educational attainment, only-child status, mode of delivery, and family history of cardiometabolic diseases. Phthalate exposures were categorized into quartiles, with the lowest quartile as the reference. OR: odds ratio; CI: confidence interval; MMP: monomethyl phthalate; MEP: monoethyl phthalate; MBP: mono-n-butyl phthalate; MEHP: mono-2-ethylhexyl phthalate; MEOHP: mono-2-ethyl-5-oxohexyl phthalate; MEHHP: mono-2-ethyl-5-hydroxyhexyl phthalate; MiBP: monoisobutyl phthalate; ∑LMWP: sum of low-molecular-weight phthalates; ∑HMWP: sum of high-molecular-weight phthalates; ∑PAEs: sum of all measured phthalate metabolites.
In contrast, more pronounced associations were observed for the persistently abnormal pattern. Higher exposure levels of several high-molecular-weight phthalate metabolites were significantly associated with increased odds of this pattern. For example, MEOHP exposure in the second and fourth quartiles was associated with higher odds of the persistently abnormal pattern (Q2 vs. Q1: OR = 3.132, 95% CI: 1.484-6.609, P = 0.003; Q4 vs. Q1: OR = 2.837, 95% CI: 1.311-6.136, P = 0.008). Similar associations were observed for MEHHP, with both Q2 and Q4 exposures significantly increasing the odds (Q2 vs. Q1: OR = 2.172, 95% CI: 1.027-4.594, P = 0.042; Q4 vs. Q1: OR = 2.508, 95% CI: 1.179-5.333, P = 0.017). In addition, MEP exposure in the third quartile was associated with increased odds of the persistently abnormal pattern (Q3 vs. Q1: OR = 2.031, 95% CI: 1.012-4.075, P = 0.046).
For mixed exposure metrics, higher cumulative exposure to high-molecular-weight phthalates (ΣHMWP) was also associated with the persistently abnormal pattern. Specifically, participants in the second and fourth quartiles had increased odds compared with those in the lowest quartile (Q2 vs. Q1: OR = 2.763, 95% CI: 1.302-5.864, P = 0.008; Q4 vs. Q1: OR = 2.258, 95% CI: 1.029-4.954, P = 0.042). Results from sensitivity analyses, including additional dietary adjustment, alternative model specifications, and alternative exposure categorization to address sparse data issues, were generally consistent with the primary findings (Supplementary Tables 5-7). Sensitivity analyses using conventional creatinine correction showed similar effect directions, although several estimates were attenuated and confidence intervals were wider. Detailed results are presented in Supplementary Table 8.
For the worsening pattern, statistically significant associations were observed for only a limited number of metabolites, and the directions of association were inconsistent. Higher exposure levels of MBP and MEHHP were associated with lower odds of the worsening pattern (MBP Q2 vs. Q1: OR = 0.583, 95% CI: 0.343-0.990, P = 0.046; MEHHP Q3 vs. Q1: OR = 0.542, 95% CI: 0.305-0.962, P = 0.037). However, most metabolites and mixed-exposure indices did not show consistent associations with this pattern, and these findings should be interpreted with caution.
Sex-stratified analyses
Sex-stratified analyses based on the fully adjusted model (Model 3) are presented in Figure 3, and quartile-specific interaction estimates (exposure × sex) are provided in Supplementary Table 9. Overall, several positive associations between phthalate exposure and the persistently abnormal cardiometabolic risk pattern were observed among boys, whereas corresponding associations among girls were generally weaker and less consistent.
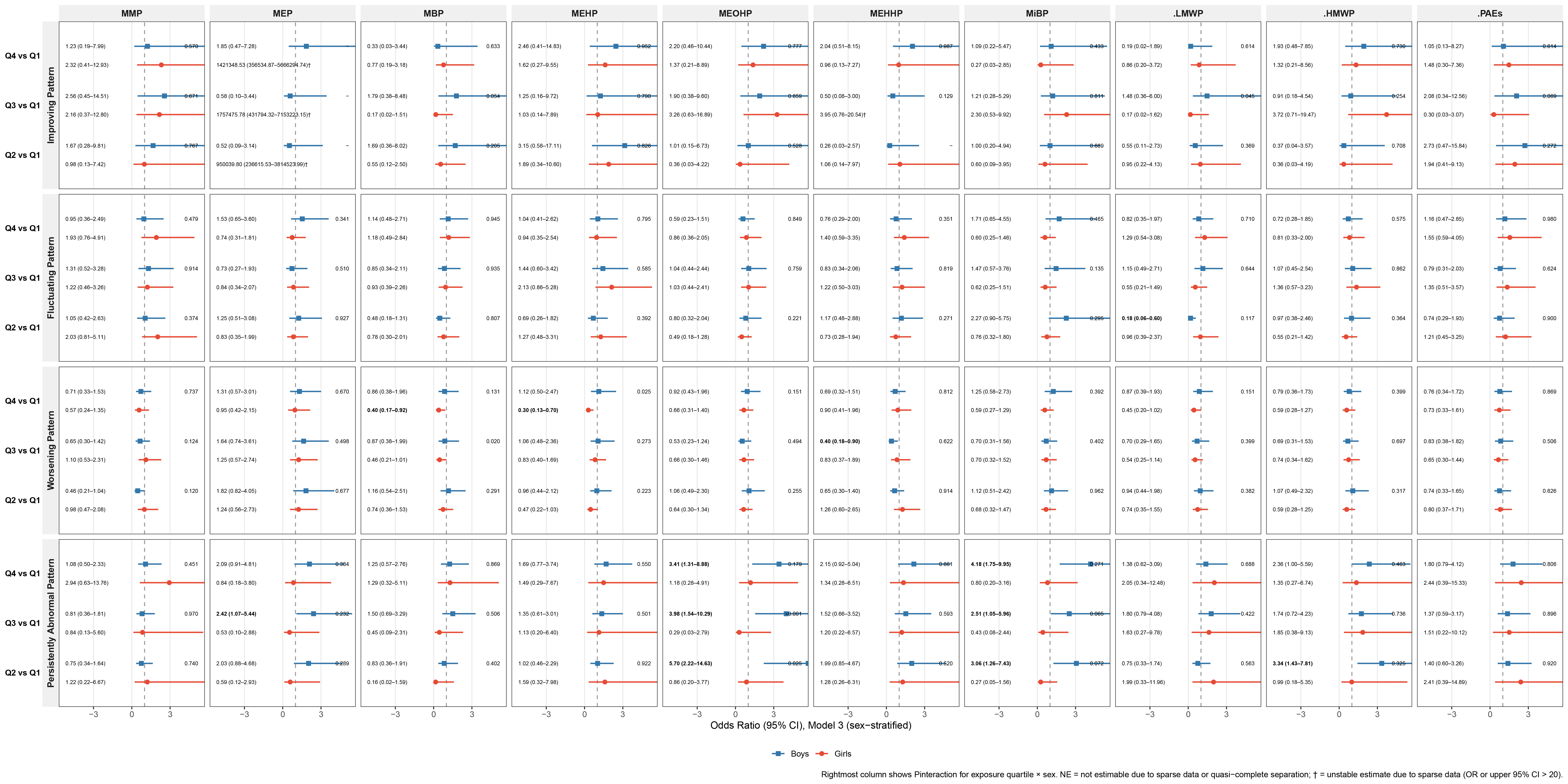
Figure 3. Sex-stratified associations between phthalate exposure and cardiometabolic risk progression patterns. Sex-stratified analyses based on multinomial logistic regression models (Model 3). Model 3 was adjusted for age, residence, parental educational attainment, only-child status, mode of delivery, and family history of cardiometabolic diseases. Phthalate exposures were categorized into quartiles. OR: Odds ratio; CI: confidence interval; MEP: monoethyl phthalate; MBP: mono-n-butyl phthalate; MEHP: mono-2-ethylhexyl phthalate; MEOHP: mono-2-ethyl-5-oxohexyl phthalate; MEHHP: mono-2-ethyl-5-hydroxyhexyl phthalate; MiBP: monoisobutyl phthalate; ∑LMWP: sum of low-molecular-weight phthalates; ∑HMWP: sum of high-molecular-weight phthalates; ∑PAEs: sum of all measured phthalate metabolites.
Among boys, higher exposure levels of several phthalate metabolites were associated with increased odds of the persistently abnormal pattern. For example, MEP exposure in the third quartile was associated with higher odds (Q3 vs. Q1: OR = 2.417, 95% CI: 1.074-5.438, P = 0.033). Similarly, MEOHP exposure across the second to fourth quartiles showed consistently elevated odds (OR range: 3.414-5.698, all P ≤ 0.012). Comparable patterns were also observed for MiBP, with Q2-Q4 exposure groups demonstrating increased odds of the persistently abnormal pattern (OR range: 2.505-4.179, all P ≤ 0.038). For mixed exposure indices, ΣHMWP exposure in the second quartile was positively associated with this pattern (Q2 vs. Q1: OR = 3.342, 95% CI: 1.430-7.809, P = 0.005).
Among girls, most associations between phthalate exposure and the persistently abnormal pattern were not statistically significant, and effect estimates were generally less stable. Formal interaction tests indicated limited statistical evidence for effect modification by sex for most metabolites [Supplementary Table 9]. Therefore, these findings should be interpreted with caution.
For the worsening pattern, only a small number of inverse associations were observed among girls, and no consistent patterns were identified across exposure metrics.
Modifying role of adherence to the 24-h movement guidelines
As shown in Figure 4, adherence to the 24-h movement guidelines varied considerably among participants. Only 23.1% of children met all three recommendations for physical activity, recreational screen time, and sleep duration, whereas 5.6% met none. The remaining participants met either one (29.8%) or two (42.8%) components.
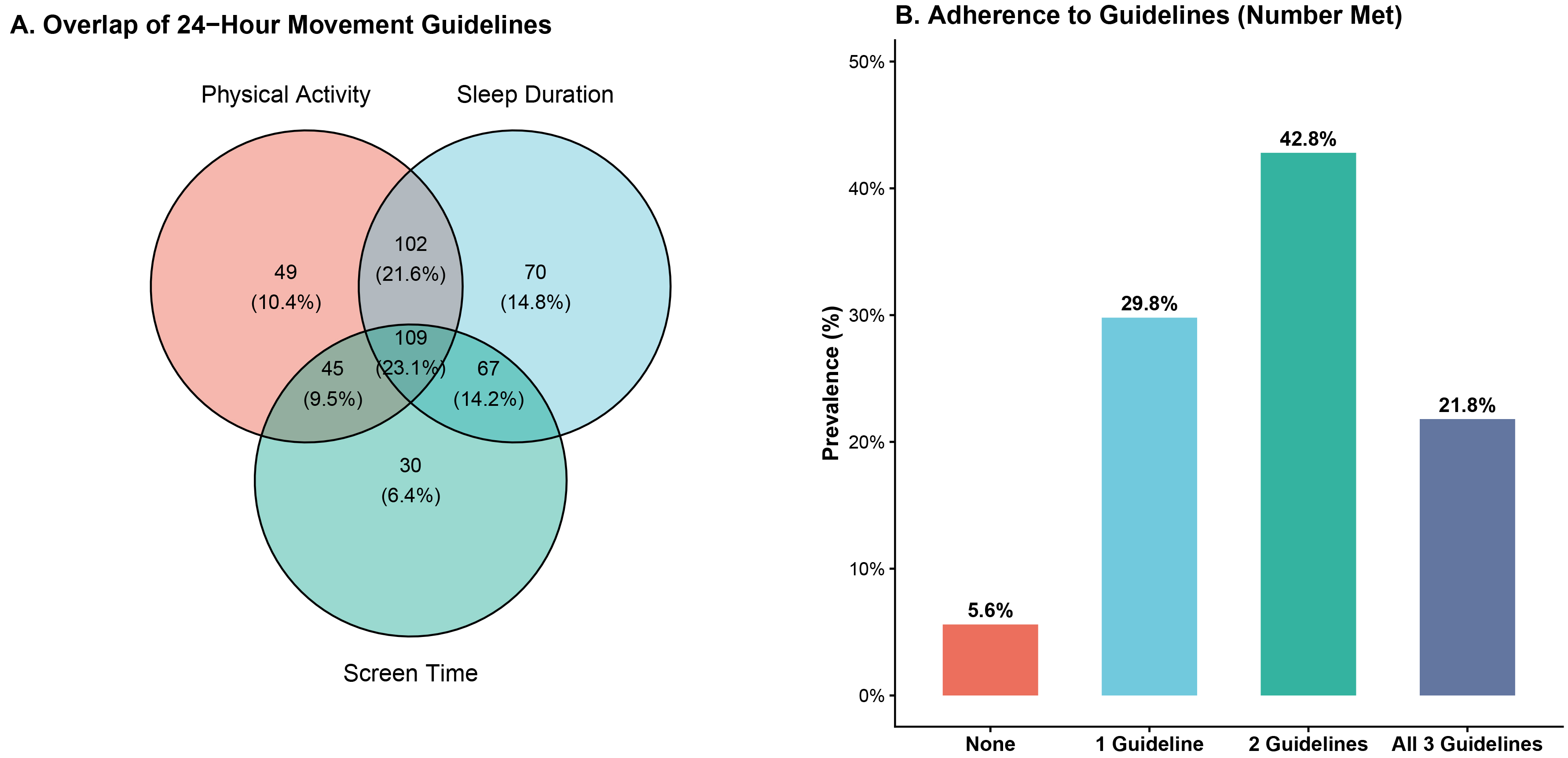
Figure 4. Distribution of adherence to the 24-h movement guidelines among participants. (A) Venn diagram showing the overlap of adherence to physical activity, recreational screen time, and sleep duration recommendations; (B) Bar chart showing the distribution of participants according to the number of 24-h movement guideline components met. Participants were classified according to the number of recommendations met (0-3), including physical activity, recreational screen time, and sleep duration.
Potential effect modification by adherence to the 24-h movement guidelines was evaluated in the fully adjusted model (Model 3) by including multiplicative interaction terms between phthalate exposure quartiles and adherence status. Overall, limited evidence of interaction was observed for several high-molecular-weight phthalate metabolites in relation to the persistently abnormal cardiometabolic risk pattern [Figure 5 and Supplementary Table 10].
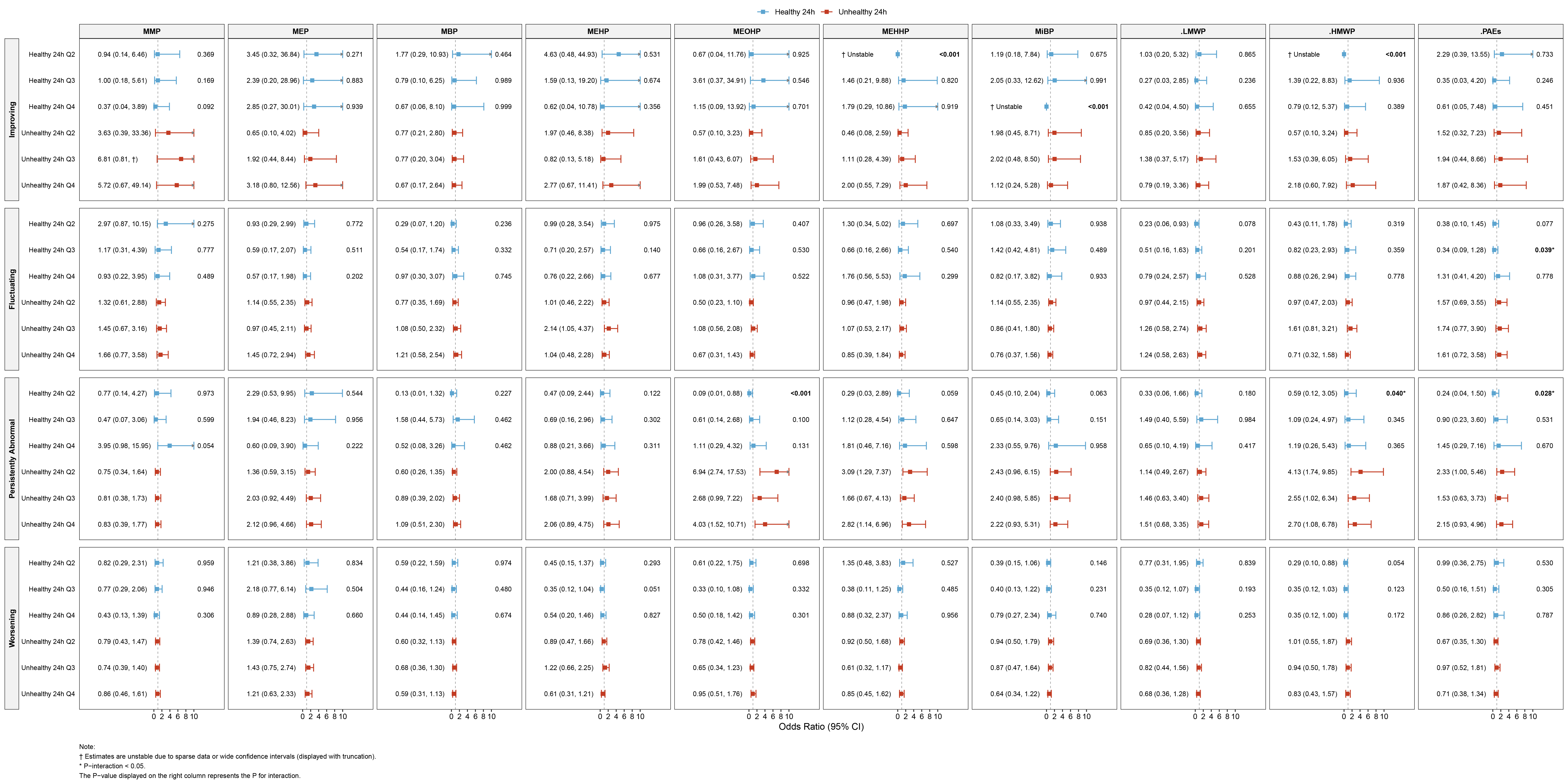
Figure 5. Interaction between phthalate exposure and adherence to 24-h movement guidelines on cardiometabolic risk progression patterns. Interaction analyses between phthalate exposure and adherence to the 24-h movement guidelines based on multinomial logistic regression models (Model 3). Model 3 was adjusted for age, sex, residence, parental educational attainment, only-child status, mode of delivery, and family history of cardiometabolic diseases. NE indicates estimates not calculable due to sparse data or model instability. OR: odds ratio; CI: confidence interval; MMP: monomethyl phthalate; MEP: monoethyl phthalate; MBP: mono-n-butyl phthalate; MEHP: mono-2-ethylhexyl phthalate; MEHHP: mono-2-ethyl-5-hydroxyhexyl phthalate; MiBP: monoisobutyl phthalate; LMWP: low-molecular-weight phthalates; HMWP: high-molecular-weight phthalates; PAE: phthalate ester.
Specifically, interaction estimates for some DEHP-related metabolites (e.g., MEOHP, MEHHP, and ΣHMWP) suggested differential associations according to adherence to the 24-h movement guidelines. However, several interaction estimates were accompanied by wide confidence intervals or extreme point estimates, likely reflecting limited sample sizes within certain exposure-behavior strata. Therefore, these findings should be interpreted cautiously.
Similar patterns were observed in additional analyses evaluating individual components of the 24-h movement guidelines separately [Supplementary Table 10], although the estimates were generally imprecise and did not consistently support strong effect modification.
Associations of phthalate mixture exposure with cardiometabolic risk progression patterns
Weighted quantile sum (WQS) regression analyses were conducted to further evaluate associations between phthalate mixture exposure and cardiometabolic risk progression patterns [Figure 6]. In the fully adjusted model, the WQS index was significantly associated with the persistently abnormal cardiometabolic risk pattern. Compared with the stable healthy pattern, each one-quartile increase in the mixture index was associated with higher odds of the persistently abnormal pattern (OR = 1.56, 95% CI: 1.05-2.33, P = 0.029).
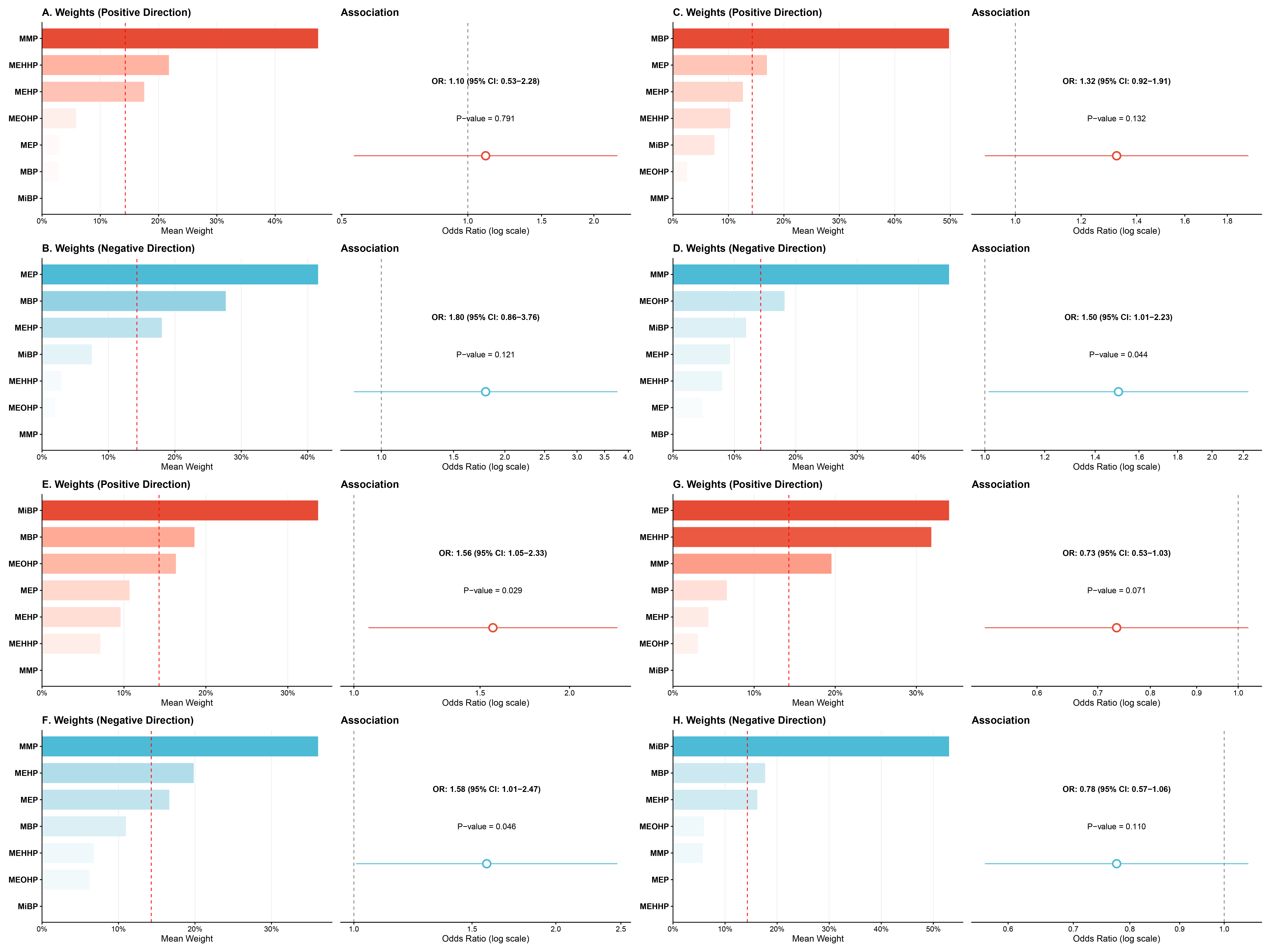
Figure 6. Weighted Quantile Sum (WQS) model of phthalate exposure and cardiometabolic risk progression patterns. Results from weighted quantile sum regression analyses are shown for both positive- and negative-direction models. (A) Positive-direction model for the improving pattern; (B) Negative-direction model for the improving pattern; (C) Positive-direction model for the fluctuating pattern; (D) Negative-direction model for the fluctuating pattern; (E) Positive-direction model for the persistently abnormal pattern; (F) Negative-direction model for the persistently abnormal pattern; (G) Positive-direction model for the worsening pattern; (H) Negative-direction model for the worsening pattern. In each panel, the left plot shows the WQS weights of individual phthalate metabolites, and the right plot shows the corresponding association estimate. Phthalate metabolites were categorized into quartiles and combined into a mixture index. The model was adjusted for the same covariates as Model 3. OR: Odds ratio; CI: confidence interval; MMP: monomethyl phthalate; MEP: monoethyl phthalate; MBP: mono-n-butyl phthalate; MEHP: mono-2-ethylhexyl phthalate; MEOHP: mono-2-ethyl-5-oxohexyl phthalate; MEHHP: mono-2-ethyl-5-hydroxyhexyl phthalate; MiBP: monoisobutyl phthalate.
The estimated mixture weights suggested that MiBP, MBP, and MEOHP contributed relatively more to the overall association. However, these weights should be interpreted cautiously because WQS regression prioritizes identifying dominant contributors within a constrained mixture model rather than estimating independent causal effects.
No statistically significant associations were observed between the mixture index and the improving, fluctuating, or worsening patterns. Overall, the mixture analysis was consistent with the single-exposure results and supports a potential role for phthalate co-exposure in the accumulation of persistent cardiometabolic risk.
DISCUSSION
Using longitudinal follow-up data, this study systematically characterized distinct progression patterns of cardiometabolic risk in children and evaluated the roles of phthalate exposure and adherence to the 24-h movement guidelines. Our findings demonstrated that childhood cardiometabolic risk is dynamic rather than static and follows heterogeneous trajectories, including stable healthy, improving, fluctuating, worsening, and persistently abnormal patterns. Among these patterns, phthalate exposure showed comparatively more consistent associations with the persistently abnormal pattern, with suggestive signals observed among boys. In addition, interaction analyses suggested that adherence to the 24-h movement guidelines may modify the association between phthalate exposure and the persistently abnormal pattern, although several estimates were imprecise and should be interpreted cautiously. Results from the WQS regression further supported a positive association between overall phthalate mixture burden and the persistently abnormal pattern.
In contrast to most previous studies that relied on cardiometabolic outcomes assessed at a single time point, the present study emphasizes the importance of interpreting childhood cardiometabolic risk from a progression-pattern perspective. Substantial evidence indicates that cardiometabolic risk factors emerging in childhood may persist across the life course and are associated with subclinical atherosclerosis, target-organ damage, and cardiovascular events in adulthood[2,32,33]. Increasing longitudinal evidence further suggests that early-life cardiometabolic trajectories, rather than single measurements, may better capture long-term cardiovascular vulnerability[34]. Single measurements may therefore underestimate cumulative cardiometabolic burden, whereas persistently abnormal profiles may represent a particularly vulnerable subgroup. In this context, our finding that phthalate exposure was more consistently associated with the persistently abnormal pattern than with improving or fluctuating patterns suggests that environmental exposures may be more relevant to the maintenance or accumulation of cardiometabolic abnormalities over time rather than to short-term fluctuations. These findings support the use of repeated measures and progression-pattern outcomes to identify more stable and clinically meaningful cardiometabolic risk phenotypes in pediatric environmental health research.
Accumulating epidemiologic evidence has linked phthalate exposure to multiple cardiometabolic risk factors in children and adolescents, including dyslipidemia, elevated blood pressure, and clustering of cardiometabolic abnormalities[10,26,35]. For example, a Chinese pediatric cohort reported positive associations between urinary phthalate metabolites and dyslipidemia, with stronger signals observed among boys[26]. A prospective cohort study in Korea similarly identified longitudinal associations between phthalate exposure and lipid profiles and insulin sensitivity indices in children[35]. In other populations, analyses from NHANES and European cohorts have reported associations between phthalate exposure and adiposity distribution, overweight, and cardiometabolic risk indicators in adolescents and adults[10,12]. Nevertheless, inconsistencies in the magnitude and direction of associations across studies remain, likely reflecting differences in follow-up duration, outcome definitions, exposure timing, and population characteristics. Some studies further suggest that associations with cardiometabolic outcomes may be more consistent for higher-molecular-weight phthalates, particularly metabolites of DEHP[8,36]. Within this context, our progression-pattern approach, which integrates information across multiple follow-up visits, highlighted a clearer association with the persistently abnormal pattern, whereas associations with improving or fluctuating patterns were comparatively weak. By incorporating longitudinal information, this approach may reduce random variability inherent to single assessments and facilitate identification of environmental exposures linked to sustained adverse cardiometabolic states.
Potential sex-specific patterns were observed in our analyses. In sex-stratified analyses, positive associations between phthalate exposure and the persistently abnormal cardiometabolic risk pattern were mainly observed among boys, whereas corresponding positive associations were not evident among girls. To formally evaluate sex-related heterogeneity, we additionally conducted sex-by-exposure interaction tests; however, these results should be interpreted cautiously, as subgroup analyses are sensitive to reduced sample size, wider confidence intervals, and potentially unstable estimates in sparse exposure-outcome cells. Similar sex-specific patterns have been reported in previous epidemiological studies, in which phthalate exposure showed stronger or more consistent associations with adiposity, dyslipidemia, and clustering of cardiometabolic risk factors among boys than among girls[11,12,26]. Several biological mechanisms may plausibly underlie these sex differences. Phthalates are well-recognized endocrine-disrupting chemicals with anti-androgenic properties, and experimental and human studies have demonstrated their capacity to interfere with sex hormone signaling during critical developmental windows[9,14,37]. Because androgen signaling plays an important role in lipid metabolism, insulin sensitivity, and body fat distribution, its disruption may lead to sex-specific metabolic effects. In addition, sex-specific differences in adipose tissue distribution may further contribute to differential cardiometabolic vulnerability, as boys tend to accumulate a higher proportion of visceral adiposity, which is metabolically active and more strongly associated with cardiometabolic risk[32,38]. Beyond endocrine-disrupting pathways, alternative explanations should also be considered. Emerging evidence suggests that boys and girls may differ in phthalate metabolism and elimination efficiency, as well as in behavioral exposure patterns (e.g., product use and activity environments). Furthermore, sex-specific developmental timing and susceptibility windows during childhood and adolescence may influence vulnerability to environmental metabolic stressors. Given the modest sample size in stratified analyses and the multiple comparisons involved, chance findings cannot be ruled out. Future studies with larger samples, repeated exposure assessment, and biomarker validation are needed to confirm whether the observed sex-specific patterns reflect true biological heterogeneity[39-41].
Importantly, our results suggest that adherence to the 24-h movement guidelines may play a modifying role in the associations between phthalate exposure and persistently abnormal cardiometabolic risk patterns, although the magnitude and consistency of interaction effects were modest. In fully adjusted models including exposure-by-lifestyle interaction terms, some evidence of effect modification was observed for several higher-molecular-weight phthalate metabolites, particularly in relation to the persistently abnormal pattern. However, several estimates were accompanied by wide confidence intervals or extreme point estimates, likely reflecting limited sample sizes within specific exposure-behavior strata. Therefore, these interaction findings should be interpreted cautiously. Phthalate exposure has been linked to increased oxidative stress, low-grade systemic inflammation, and dysregulation of glucose and lipid metabolism - pathways central to the development and maintenance of cardiometabolic abnormalities[8,13,15]. In contrast, regular physical activity has been shown to improve insulin sensitivity, reduce systemic inflammation, and promote favorable lipid metabolism, potentially counteracting phthalate-induced metabolic disturbances[16,17,42]. Adequate sleep duration represents another key component of metabolic homeostasis, influencing hormonal regulation, circadian rhythm stability, and glucose metabolism. Insufficient sleep has been associated with increased cardiometabolic risk and may exacerbate susceptibility to environmental metabolic stressors[43,44]. Excessive recreational screen time, conversely, is closely linked to sedentary behavior, sleep disruption, and adverse metabolic profiles. When conceptualized as an integrated behavioral composition, adherence to the 24-h movement guidelines may reflect overall physiological resilience rather than acting as a direct protective factor against specific environmental exposures. Previous studies have similarly suggested that healthy lifestyle behaviors may modify the associations between environmental pollutant exposures and cardiometabolic outcomes, although findings remain heterogeneous across populations and exposure contexts[19,45]. Taken together, our results provide suggestive - but not definitive - evidence that favorable movement behaviors may partially mitigate environmentally related cardiometabolic risks during childhood, highlighting the importance of integrated prevention strategies while underscoring the need for further longitudinal and mechanistic research.
Beyond single-chemical and interaction analyses, we applied WQS regression to evaluate the joint effects of multiple phthalate metabolites as a mixture. The WQS index was positively associated with the persistently abnormal cardiometabolic risk pattern, whereas no statistically significant associations were observed for the improving, fluctuating, or worsening patterns. These findings suggest that cumulative phthalate exposure may be more relevant to the maintenance of long-term adverse cardiometabolic profiles rather than to short-term dynamic changes. Notably, the negative-direction WQS model also yielded statistically significant associations for certain outcome patterns, indicating potential heterogeneity in the direction of effects across individual phthalate metabolites. This observation suggests that mixture effects may not be strictly unidirectional. Therefore, these findings should be interpreted cautiously in light of the directional constraints inherent to the WQS approach. Several higher-molecular-weight phthalate metabolites contributed most strongly to the mixture index, which is consistent with prior evidence suggesting that DEHP-related metabolites may exert more pronounced metabolic effects compared with lower-molecular-weight phthalates[25, 46]. However, mixture effect estimates should be interpreted with caution, as WQS regression assumes a common directional effect across components and may be sensitive to correlations among exposures. In addition, uncertainty in weight estimates and limited statistical power for certain progression patterns may partly explain the lack of consistent associations across all trajectory categories. Taken together, these results highlight the importance of considering chemical mixtures when evaluating environmental cardiometabolic risk in children. While single-compound analyses may underestimate the cumulative burden of concurrent exposures, mixture-based approaches provide complementary insights into real-world exposure complexity.
This study has several strengths. First, the use of longitudinal follow-up data and progression-pattern outcomes allowed identification of more stable and public health-relevant cardiometabolic risk profiles. Second, the integration of single-metabolite analyses, sex-stratified analyses, interaction analyses, and mixture modeling provided complementary evidence across multiple analytic dimensions. Third, the incorporation of the 24-h movement guidelines highlighted the importance of considering modifiable lifestyle behaviors alongside environmental exposures. Several limitations should also be acknowledged. First, participants were predominantly urban school-aged children from Xiamen, a southeastern coastal city in China. Although this urban-based cohort provides valuable insight into cardiometabolic risk development under rapidly changing environmental and lifestyle contexts, the findings may not be fully generalizable to rural populations or regions with substantially different exposure profiles and socioeconomic conditions. Second, urinary phthalate metabolites reflect relatively short-term exposure and exhibit considerable within-person variability. Although repeated measurements between 2018 and 2020 were used to approximate habitual exposure, these indicators cannot fully capture long-term exposure. Furthermore, detailed information on exposure sources, such as dietary intake, indoor environmental factors, and product use, was not available, which may have contributed to exposure misclassification. Third, adherence to the 24-h movement guidelines was assessed using questionnaire-based measures and may therefore be subject to recall and social desirability bias. Some interaction estimates were accompanied by wide confidence intervals, likely reflecting limited sample sizes within certain exposure-behavior strata. Moreover, because both exposure and lifestyle measures are subject to measurement error, interaction estimates may be biased and should be interpreted cautiously. Fourth, although multiple sociodemographic and developmental factors were adjusted for, residual confounding cannot be completely excluded. In particular, pubertal transition during follow-up may have influenced cardiometabolic trajectories. While participants were within a relatively narrow age range at baseline, repeated assessments of pubertal stage were not consistently available, and time-varying adjustment for pubertal development was therefore not feasible. Finally, cardiometabolic risk status was defined as the presence of any individual abnormality, which may obscure differences in severity, clustering patterns, or cumulative burden. Alternative analytical approaches, such as trajectory modeling or composite risk scoring, may provide more refined characterization in future research.
In conclusion, using repeated follow-up data, this study highlights the dynamic nature of cardiometabolic risk development during childhood and identifies a relatively consistent association between phthalate exposure and the persistently abnormal cardiometabolic risk pattern, particularly among boys. While associations with improving or fluctuating patterns were generally weaker and less consistent, the observed relationship with sustained cardiometabolic abnormalities suggests that environmental chemical exposures may contribute more to the maintenance or accumulation of cardiometabolic risk rather than short-term variation. Evidence of effect modification by adherence to the 24-h movement guidelines was observed, although these findings should be interpreted cautiously given the imprecision of some subgroup estimates. Mixture analyses further supported a positive association between overall phthalate exposure burden and the persistently abnormal pattern. Together, these findings underscore the potential importance of jointly addressing environmental chemical exposures and modifiable lifestyle behaviors in early-life strategies aimed at preventing long-term cardiometabolic risk in children.
DECLARATIONS
Acknowledgments
We sincerely thank the project team members, schoolteachers, investigators, and all students, parents, and local education and health staff who contributed to the study.
Authors’ contributions
Conceptualized and designed the study, performed statistical analyses, drafted the initial manuscript, and reviewed and revised the manuscript: Wang R
Contributed to the study's conceptualization and design, supervised data collection, statistical analyses, and initial drafting of the manuscript, and reviewed and revised the manuscript: Song X, Jiang J, Song Z, Dong Y
Assisted with data interpretation and contributed to the revision of the manuscript: Zhang Y, Liu J, Dong Z, Qin Y, Zhang D, Lu Z, Chen L, Liang J
Reviewed and revised the manuscript: Dong Y, Ma J, Song Y
All authors approved the final manuscript as submitted and agreed to be accountable for all aspects of the work.
AI and AI-assisted tools statement
During the preparation of this manuscript, the AI tool Gemini 3 Pro Preview (Google, released 2025-11-18) was used to assist in generating the graphical abstract. The tool was used solely for visual illustration and did not influence the study design, data collection, analysis, interpretation, or the scientific content of the work. All authors take full responsibility for the accuracy, integrity, and final content of the manuscript.
Availability of data and materials
The datasets supporting the results of this study are not openly accessible due to privacy concerns. However, they can be obtained from the corresponding author upon reasonable request.
Financial support and sponsorship
The present study was supported by the National Key R&D Program of China (2024YFC3308302 to Dong Y), the National Natural Science Foundation of China (82103865 and 82373593 to Dong Y), the Beijing Natural Science Foundation (7222244 to Dong Y), and the Peking University Talent Introduction Program Project (BMU2023YJ011 to Dong Y).
Conflicts of interest
Song Y is the Guest Editor of the Special Issue entitled “Metabolic Heterogeneity in Childhood Obesity and Preventive Strategy” in the journal Metabolism and Target Organ Damage. Song Y was not involved in any steps of editorial processing, notably including reviewers’ selection, manuscript handling, or decision-making. The other authors declare that there are no conflicts of interest.
Ethical approval and consent to participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Medical Ethics Committee of Peking University (approval number: IRB00001052-17026). Written informed consent was obtained from all participants and their legal guardians prior to enrollment.
Consent for publication
Not applicable.
Copyright
© The Author(s) 2026.
Supplementary Materials
REFERENCES
1. Juonala M, Magnussen CG, Berenson GS, et al. Childhood adiposity, adult adiposity, and cardiovascular risk factors. N Engl J Med. 2011;365:1876-85.
3. Bjerregaard LG, Adelborg K, Baker JL. Change in body mass index from childhood onwards and risk of adult cardiovascular disease,. Trends Cardiovasc Med. 2020;30:39-45.
4. Wang G, Wei D, Kebede Merid S, et al. BMI trajectories from birth to young adulthood associate with distinct cardiometabolic profiles. BMC Med. 2024;22:510.
5. O'keeffe LM, Tilling K, Bell JA, et al. Sex-specific trajectories of molecular cardiometabolic traits from childhood to young adulthood. Heart. 2023;109:674-85.
6. Callo Quinte G, Barros F, Gigante DP, De Oliveira IO, Dos Santos Motta JV, Horta BL. Overweight trajectory and cardio metabolic risk factors in young adults. BMC Pediatr. 2019;19:75.
7. Norris T, Mansukoski L, Gilthorpe MS, et al. Distinct body mass index trajectories to young-adulthood obesity and their different cardiometabolic consequences. Arterioscler, Thromb, Vasc Biol. 2021;41:1580-93.
8. Golestanzadeh M, Riahi R, Kelishadi R. Association of exposure to phthalates with cardiometabolic risk factors in children and adolescents: a systematic review and meta-analysis. Environ Sci Pollut Res. 2019;26:35670-86.
9. Haverinen E, Fernandez MF, Mustieles V, Tolonen H. Metabolic syndrome and endocrine disrupting chemicals: an overview of exposure and health effects. Int J Environ Res Public Health. 2021;18:13047.
10. Webb MD, Park JW, Day DB, Trabulsi JC, Sathyanarayana S, Melough MM. Associations of phthalate exposure with adiposity and metabolic syndrome in us adolescents and adults, NHANES 2013 to 2018. J Endocr Soc. 2024;8:bvae189.
11. Vafeiadi M, Myridakis A, Roumeliotaki T, et al. Association of early life exposure to phthalates with obesity and cardiometabolic traits in childhood: sex specific associations. Front. Public Health. 2018;6:327.
12. Berghuis SA, Bocca G, Bos AF, et al. Adolescent urinary concentrations of phthalate metabolites and indices of overweight and cardiovascular risk in Dutch adolescents. Environ Int. 2024;194:109167.
13. Tian Y, Xu M, Shang H, et al. Differential disruption of glucose and lipid metabolism induced by phthalates in human hepatocytes and white adipocytes. Toxics. 2024;12:214.
14. Alahmadi H, Martinez S, Farrell R, et al. Mixtures of phthalates disrupt expression of genes related to lipid metabolism and peroxisome proliferator-activated receptor signaling in mouse granulosa cells. Pharmacol. Toxicol. 2024.
15. Ferguson KK, Cantonwine DE, Rivera-González LO, et al. Urinary phthalate metabolite associations with biomarkers of inflammation and oxidative stress across pregnancy in Puerto Rico. Environ Sci Technol. 2014;48:7018-25.
16. Tremblay MS, Carson V, Chaput J, et al. Canadian 24-hour movement guidelines for children and youth: an integration of physical activity, sedentary behaviour, and sleep. Appl Physiol Nutr Metab. 2016;41 Suppl:S311-27.
17. Rollo S, Antsygina O, Tremblay MS. The whole day matters: Understanding 24-hour movement guideline adherence and relationships with health indicators across the lifespan. J Sport Health Sci. 2020;9:493-510.
18. Carrico C, Gennings C, Wheeler DC, Factor-litvak P. Characterization of weighted quantile sum regression for highly correlated data in a risk analysis setting. JABES. 2014;20:100-20.
19. Braun JM, Papandonatos GD, Li N, et al. Physical activity modifies the relation between gestational perfluorooctanoic acid exposure and adolescent cardiometabolic risk. Environ Res. 2022;214:114021.
20. Silva M, Samandar E, Preaujr J, Reidy J, Needham L, Calafat A. Quantification of 22 phthalate metabolites in human urine☆. J Chromatogr B. 2007;860:106-12.
21. Dong Y, Chen L, Gao D, et al. Endogenous sex hormones homeostasis disruption combined with exogenous phthalates exposure increase the risks of childhood high blood pressure: A cohort study in China. Environ Int. 2022;168:107462.
22. Dong Y, Gao D, Li Y, et al. Effect of childhood phthalates exposure on the risk of overweight and obesity: a nested case-control study in China. Environ Int. 2022;158:106886.
23. Ye X, Kuklenyik Z, Needham LL, Calafat AM. Automated on-line column-switching HPLC-MS/MS method with peak focusing for the determination of nine environmental phenols in urine. Anal Chem. 2005;77:5407-13.
24. Barr DB, Wilder LC, Caudill SP, Gonzalez AJ, Needham LL, Pirkle JL. Urinary creatinine concentrations in the U.S. population: implications for urinary biologic monitoring measurements. Environ Health Perspect. 2005;113:192-200.
25. O’brien KM, Upson K, Cook NR, Weinberg CR. Environmental chemicals in urine and blood: improving methods for creatinine and lipid adjustment. Environ Health Perspect. 2016;124:220-7.
26. Gao D, Zou Z, Li Y, et al. Association between urinary phthalate metabolites and dyslipidemia in children: results from a Chinese cohort study. Environ Pollut. 2022;295:118632.
27. Cook S, Weitzman M, Auinger P, Nguyen M, Dietz WH. Prevalence of a metabolic syndrome phenotype in adolescents: findings from the third national health and nutrition examination survey, 1988-1994. Arch Pediatr Adolesc Med. 2003;157:821.
28. Zimmet P, Alberti KGM, Kaufman F, et al. ; IDF Consensus Group. The metabolic syndrome in children and adolescents? an IDF consensus report. Pediatr Diabetes. 2007;8:299-306.
29. National Health Commission of the People’s Republic of China. High waist circumference screening threshold among children and adolescents aged 7 ~ 18 years. Available from: http://www.nhc.gov.cn/wjw/pqt/201807/417de6982ab8493b91aba925b51a8a19.shtml. [Accessed on 18 Dec 2025].
30. National Health Commission of the People’s Republic of China. Screening threshold for high blood pressure among children and adolescents aged 7-18 years. Available from: https://www.nhc.gov.cn/wjw/pqt/201807/6cee88c1d050493ab50a411a2978f901.shtml. [Accessed on 19 Dec 2025].
31. World Health Organization. Guidelines on physical activity, sedentary behaviour and sleep for children under 5 years of age: World Health Organization; 2019. Available from: https://www.bing.com/ck/a?!&&p=6c137ea3bd2d6d148175c2464e1dcf0c9a1f13dcad229ec2380425ebe747aae5JmltdHM9MTc3OTQwODAwMA&ptn=3&ver=2&hsh=4&fclid=220b64ac-4f94-69d6-2323-73cd4e53681f&u=a1aHR0cHM6Ly93d3cud2hvLmludC9wdWJsaWNhdGlvbnMvaS9pdGVtLzk3ODkyNDE1NTA1MzY. [Accessed on 22 May 2026].
32. Raitakari OT, Juonala M, Kähönen M, et al. Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood: the cardiovascular risk in young Finns study. JAMA. 2003;290:2277.
33. Li S, Chen W, Srinivasan SR, et al. Childhood cardiovascular risk factors and carotid vascular changes in adulthood: the Bogalusa heart study. JAMA. 2003;290:2271.
34. Allen NB, Krefman AE, Labarthe D, et al. Cardiovascular health trajectories from childhood through middle age and their association with subclinical atherosclerosis. JAMA Cardiol. 2020;5:557.
35. Han H, Lee HA, Park B, et al. Associations of phthalate exposure with lipid levels and insulin sensitivity index in children: a prospective cohort study. Sci Total Environ. 2019;662:714-21.
36. Trasande L, Attina TM, Sathyanarayana S, Spanier AJ, Blustein J. Race/Ethnicity-specific associations of urinary phthalates with childhood body mass in a nationally representative sample. Environ Health Perspect. 2013;121:501-6.
37. Ferguson KK, Peterson KE, Lee JM, et al. Prenatal and peripubertal phthalates and bisphenol A in relation to sex hormones and puberty in boys. Reprod Toxicol. 2014;47:70-6.
38. O’Keeffe LM, Tilling K, Bell JA, Walsh PT, Lee MA, Lawlor DA, et al. Sex-specific trajectories of molecular cardiometabolic traits from childhood to young adulthood. Heart. 2023;109:674-85.
39. Demir A, Aydin A, Büyükgebiz A. Thematic review of endocrine disruptors and their role in shaping pubertal timing. Children. 2025;12:93.
40. Yu Z, Mo H, Shan C, et al. Risk of neurodevelopmental disorders in preschool children associated with the longitudinal trajectory of phthalates during pregnancy: potential mechanisms based on metabonomics of cord blood. Environ Sci Technol. 2025;59:16180-92.
41. Gao K, Hua K, Chen X, et al. Occurrence, characteristics, and mixed reproductive exposure risk assessment of traditional phthalates and their novel alternatives in campus indoor dust. Environ Sci Technol. 2025;59:6708-18.
42. Bull FC, Al-ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. 2020;54:1451-62.
43. Chaput J, Gray CE, Poitras VJ, et al. Systematic review of the relationships between sleep duration and health indicators in school-aged children and youth. Appl Physiol Nutr Metab. 2016;41 Suppl:S266-82.
44. Buxton OM, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Social Science & Medicine. 2010;71:1027-36.
45. Guo T, Zhang Y, Chen L, et al. The role of lifestyle in the impact of constant phthalate exposure on overweight and obesity: a longitudinal cohort study in China. Pediatric Obesity. 2025;20:e70011.
Cite This Article
How to Cite
Download Citation
Export Citation File:
Type of Import
Tips on Downloading Citation
Citation Manager File Format
Type of Import
Direct Import: When the Direct Import option is selected (the default state), a dialogue box will give you the option to Save or Open the downloaded citation data. Choosing Open will either launch your citation manager or give you a choice of applications with which to use the metadata. The Save option saves the file locally for later use.
Indirect Import: When the Indirect Import option is selected, the metadata is displayed and may be copied and pasted as needed.
About This Article
Special Topic
Copyright

Data & Comments
Data
0













Comments
Comments must be written in English. Spam, offensive content, impersonation, and private information will not be permitted. If any comment is reported and identified as inappropriate content by OAE staff, the comment will be removed without notice. If you have any queries or need any help, please contact us at [email protected].