


fig2
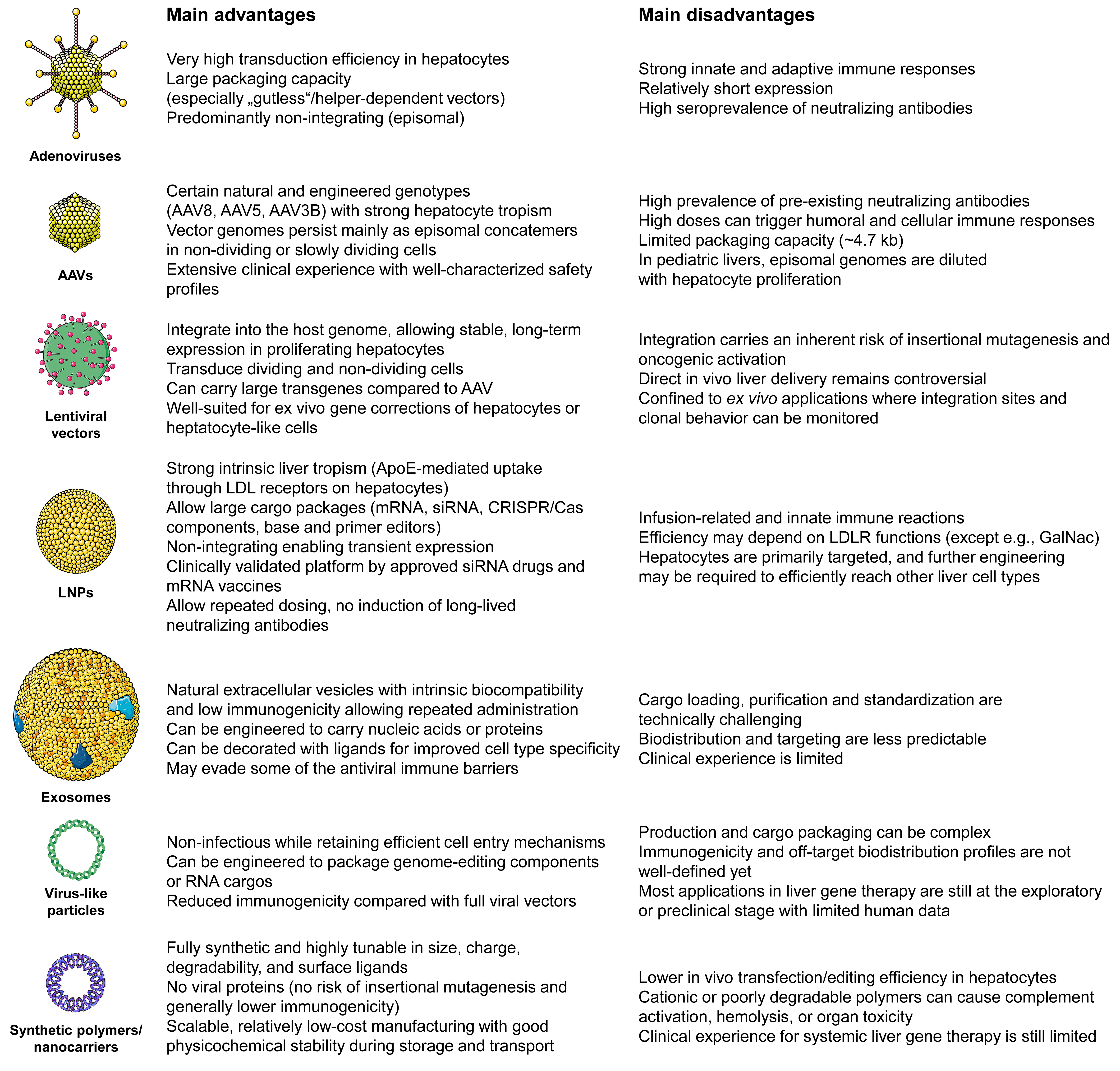
Figure 2. Comparison of different delivery platforms for liver-directed gene therapy. The figure highlights the main advantages and disadvantages of adenoviral vectors, adeno-associated virus (AAVs) vectors, lentiviral vectors, lipid nanoparticles (LNPs), exosomes, virus-like particles, and synthetic polymers/nanocarriers for hepatic gene transfer. Adenoviral vectors and AAVs are known for achieving high transduction efficiency in hepatocytes. Specific AAV serotypes like AAV8, AAV5, and AAV3B demonstrate strong liver tropism. However, they are constrained by immunogenicity, high seroprevalence of neutralizing antibodies, limited packaging capacity, and loss of episomal genomes in proliferating pediatric livers in the case of AAVs. Lentiviral vectors integrate into the host genome and can carry larger cassettes, enabling stable, long-term expression. This feature makes them suitable for ex vivo gene correction of hepatocytes or hepatocyte-like cells. Nevertheless, the risk of insertional mutagenesis and oncogenic activation currently restricts their direct in vivo liver applications. Non-viral systems, such as LNPs, exosomes, virus-like particles, and synthetic polymers/nanocarriers, have the ability to deliver mRNA, siRNA, and genome-editing components (such as CRISPR-Cas-based nucleases, base editors, and prime editors) with adaptable cargo size. They also offer the potential for repeated administration. However, they encounter challenges related to innate immune activation, reliance on LDLR-mediated uptake (for standard LNPs), cell-type specificity beyond hepatocytes, manufacturing complexity, and relatively limited clinical experience in systemic liver gene therapy.





